Surgical Infections & Tropical Surgery
Surgical infections and tropical surgery revision notes for MS/DNB General Surgery: gas gangrene, necrotising fasciitis, Fournier gangrene, C. diff, MRSA, cervical TB, mycetoma, typhoid, amoebiasis, ascariasis, hydatid disease, and intestinal TB.
Gas Gangrene (Clostridial Myonecrosis)
►Definition
Gas gangrene is an acute, rapidly progressive, life-threatening necrotising infection of skeletal muscle caused by toxin-producing anaerobic spore-forming bacteria of the genus Clostridium. It is characterised by widespread myonecrosis, gas production in tissues, profound systemic toxaemia, and high mortality.
Etiology
- Causative Organisms (Obligate Anaerobes):
- Clostridium perfringens — most common (~80% of cases).
- Clostridium septicum — frequently associated with spontaneous gas gangrene, colonic malignancies, or neutropenia.
- Clostridium histolyticum, Clostridium novyi, Clostridium sporogenes.
- Predisposing Factors:
- Traumatic wounds with devitalised tissue, crush injuries, compound fractures.
- Postoperative wounds, septic abortions, and accidental intramuscular (IM) injections.
- Ischemic tissue conditions (peripheral arterial disease, diabetes, malignancy, and immunosuppression).
- Spontaneous gangrene (especially C. septicum) in patients with occult colonic carcinoma or leukemia.
Pathophysiology
The alpha-toxin and theta-toxin work synergistically to destroy surrounding healthy muscle fibers, propagate local tissue hypoxia, and poison the systemic circulation, driving the patient into cardiovascular collapse.
Clinical Features
- Onset: Hyperacute, rapid incubation period (usually 6–48 hours after injury).
- Local Signs:
- Sudden, severe, progressive local pain disproportionate to early physical findings.
- Rapid swelling, tense local edema, and crepitus (palpable gas bubbles in subcutaneous tissues and muscle).
- Skin discoloration: progresses from pale/erythematous to bronze, then dusky blue/black, with tense blisters containing thin, dark fluid.
- Foul discharge: a thin, dark, sweetly foul-smelling exudate ("dishwater" fluid).
- Muscle appearance: non-viable, dark red/black, non-contractile, and fails to bleed when cut.
- Systemic Signs: High-grade fever, disproportionate tachycardia, tachypnea, severe systemic toxemia, rapid intravascular hemolysis, jaundice, hypotension, and acute oliguric renal failure leading to death if untreated.
Investigations
- Gram Stain of Exudate: Demonstrates large, Gram-positive bacilli with a characteristic and striking absence of polymorphonuclear leukocytes (white blood cells), which are completely destroyed by clostridial toxins.
- Plain X-ray: Shows gas in muscle planes (streaky, feathered gas bubbles outlining the muscle fascicles, not confined to fascial planes).
- CT/MRI: Delineates the exact extent of gas and muscle group involvement.
- Laboratory: Intravascular hemolysis, metabolic acidosis, elevated creatine kinase (CK), and acute renal dysfunction.
Differential Diagnosis
- Necrotising Fasciitis: Primarily involves the fascia and subcutaneous tissue; muscle is initially spared, crepitus is less common, and tissue is wooden-hard.
- Cellulitis with gas-forming organisms: Caused by E. coli, Klebsiella, or mixed aerobes; lacks the severe myonecrosis and profound systemic toxemia of gas gangrene.
- Non-infectious subcutaneous emphysema: Traumatic or iatrogenic introduction of air; lacks any signs of inflammation or systemic toxicity.
Management
-
Aggressive Resuscitation:High-flow oxygen, aggressive IV fluid resuscitation, correction of acidosis, and blood transfusions for hemolysis. Close hemodynamic monitoring in an intensive care setting is mandatory.
-
Immediate Antibiotic Therapy:Start high-dose IV Penicillin G (3–4 million units q4h) combined with IV Clindamycin (900 mg q8h) to directly inhibit bacterial toxin synthesis. Add broad-spectrum coverage (e.g., Meropenem or Piperacillin-Tazobactam) for polymicrobial coverage.
-
Emergency Surgical Debridement:The cornerstone of treatment. Immediate, radical excision of all necrotic and non-viable muscle groups (myectomy) until healthy, bleeding muscle margins are reached. Amputation of limbs is often lifesaving. Scheduled re-exploration is required in 24 hours.
-
Adjunctive Therapies:Hyperbaric Oxygen Therapy (HBOT) improves tissue oxygenation, inhibits anaerobic growth, stops clostridial toxin production, and enhances neutrophil function. Clostridial antiserum (antitoxin) is historical and rarely used now.
Prognosis
Mortality remains 15–30% even with early treatment and approaches 100% if untreated. The prognosis is worse in patients with spontaneous gas gangrene (C. septicum), delayed surgical intervention, underlying malignancy, or immunocompromised states.
Gas Gangrene vs. Necrotising Fasciitis
| Feature | Gas Gangrene (Clostridial Myonecrosis) | Necrotising Fasciitis (NF) |
|---|---|---|
| Primary Site | Skeletal muscle parenchyma primarily | Fascia and subcutaneous tissue primarily |
| Etiology | Clostridium species (esp. C. perfringens, C. septicum) | Polymicrobial (Type I) or Monomicrobial (Type II - Strep) |
| Predisposing Factors | Traumatic/war wounds, crush injuries, ischemia, malignancy (C. septicum) | Minor trauma, post-surgery, perineal sepsis (Fournier's), diabetes |
| Onset | Rapid (6–48 hours after injury) | Slower (days), but can accelerate rapidly |
| Pain | Sudden, severe, out of proportion to wound findings | Severe, disproportionate to wound; rapidly progressive |
| Local Findings | Edema, crepitus, bronze/black skin, thin foul "dishwater" fluid, non-bleeding muscle | Wooden-hard subcutaneous tissue, dusky erythema, bullae, muscle spared early |
| Exudate | Thin, dark, sweetly foul-smelling, often scant | Thick, gray "dishwater" pus, foul odor |
| Systemic Features | Severe toxemia, hemolysis, jaundice, early shock | Septicemia, septic shock, multi-organ failure late |
| Imaging | X-ray: gas in muscle planes | X-ray/CT: gas in fascia/subcutaneous tissue |
| Histopathology | Muscle necrosis, organisms in tissue, few/no neutrophils | Fascial necrosis, thrombosed vessels, polymorphous inflammatory infiltrate |
| Diagnosis | Clinical + Gram stain (Gram-positive rods, no neutrophils) | Clinical + imaging (CT/MRI), Gram stain/culture |
| Treatment | Emergency radical debridement/amputation + high-dose penicillin + clindamycin | Aggressive surgical debridement + broad-spectrum antibiotics (carbapenem + clindamycin + vancomycin) |
| Mortality | 15–30% with treatment; ~100% if untreated | 20–40% (higher in delayed diagnosis or Fournier's) |
Necrotising Fasciitis
►Definition
Necrotising fasciitis (NF) is a rapidly progressive, life-threatening destructive infection of the subcutaneous tissue and superficial fascial planes. It is characterised by microvascular thrombosis of perforating vessels, causing extensive necrosis of the fascia and overlying skin, accompanied by severe systemic toxicity.
Classification
| Type | Causative Organisms | Common Setting | Comments |
|---|---|---|---|
| Type I (Polymicrobial) | Mixed aerobic and anaerobic (Streptococcus, Staphylococcus, Enterobacteriaceae, Bacteroides) | Postoperative wounds, diabetics, obese, and immunocompromised hosts | Most common type (~80% of cases) |
| Type II (Monomicrobial) | Group A Beta-haemolytic Streptococcus (flesh-eating bacteria) ± Staphylococcus aureus | Healthy individuals, post-minor trauma or surgery | Often associated with Toxic Shock Syndrome |
| Type III (Marine/Gas) | Clostridium perfringens or Vibrio vulnificus | Marine exposure, contaminated wounds, seafood handling | Gas-forming; extremely fulminant |
| Type IV (Fungal) | Fungal (e.g., Candida, Mucor, Rhizopus) | Immunocompromised hosts, burns, major trauma | Very rare |
Etiopathology
- Predisposing Factors: Diabetes mellitus (most common), peripheral vascular disease, immunosuppression, chronic renal or hepatic failure, recent surgery or trauma, IV drug use, decubitus ulcers, and insect bites.
- Pathophysiology: Entry of organisms through minor trauma or wound → Bacterial proliferation in poorly vascularized subcutaneous tissue → Release of bacterial toxins and enzymes (streptokinase, hyaluronidase, DNase, exotoxins) → Thrombosis of perforating vessels, leading to fascia necrosis and skin ischemia.
Clinical Features
- Local Signs:
- Severe pain disproportionate to visible findings (earliest hallmark).
- Erythema progressing to dusky discoloration, followed by skin necrosis and blistering.
- "Wooden-hard" induration of the subcutaneous tissue extending beyond the margins of erythema.
- Crepitus (in gas-forming polymicrobial or clostridial infections).
- Rapid progression (measured in centimeters per hour).
- Loss of sensation over the necrotic skin (due to thrombosis and nerve destruction).
- Systemic Signs: High-grade fever, tachycardia, hypotension, septic shock, and multi-organ dysfunction syndrome (MODS) in advanced stages.
Sites of Involvement
Perineum and genitalia (Fournier's gangrene), abdominal wall (Meleney's synergistic gangrene), extremities (diabetics, IV drug users), and neck (Ludwig's angina).
LRINEC (Laboratory Risk Indicator for Necrotising Fasciitis) Score
A scoring tool used to distinguish necrotising fasciitis from simple cellulitis. A score ≥6 raises suspicion; a score ≥8 indicates a very high risk.
| Parameter | Value | Points |
|---|---|---|
| C-Reactive Protein (CRP) | <150 mg/L | 0 |
| ≥150 mg/L | 4 | |
| White Blood Cell Count (WBC) | <15,000 /mm³ | 0 |
| 15,000–25,000 /mm³ | 1 | |
| ≥25,000 /mm³ | 2 | |
| Haemoglobin (Hb) | >13.5 g/dL | 0 |
| 11–13.5 g/dL | 1 | |
| <11 g/dL | 2 | |
| Sodium (Na) | ≥135 mEq/L | 0 |
| <135 mEq/L | 2 | |
| Creatinine | <1.6 mg/dL (141 μmol/L) | 0 |
| ≥1.6 mg/dL | 2 | |
| Glucose | <180 mg/dL (10 mmol/L) | 0 |
| ≥180 mg/dL | 1 |
Differential Diagnosis
- Cellulitis: Lacks the severe pain out of proportion, systemic toxicity, and wooden-hard induration; responds well to simple antibiotics.
- Abscess: Localised, fluctuant swelling; lacks the rapid spreading necrosis along fascial planes.
- Gas Gangrene: Involves the muscle parenchyma primarily; Gram stain shows Gram-positive rods with no neutrophils.
- Erysipelas: Superficial cellulitis with well-demarcated raised borders.
Management
-
Resuscitation:Aggressive fluid resuscitation, correction of electrolyte imbalance, hemodynamic monitoring, and supportive ICU care.
-
Broad-Spectrum Antibiotics (Empirical):Start immediately: Carbapenem (e.g., Meropenem) or Piperacillin-Tazobactam, PLUS Clindamycin (to inhibit toxin production), PLUS Vancomycin or Linezolid (for MRSA coverage). Adjust based on culture results.
-
Surgical Debridement (Cornerstone):Must not be delayed. Perform early, wide surgical debridement of all necrotic fascia and subcutaneous tissue until healthy bleeding margins are reached. Multiple re-debridements are performed every 24–48 hours. Keep the wound open; use negative pressure wound therapy (VAC) and reconstruct with skin grafts or flaps later.
-
Adjunctive Therapies:Hyperbaric Oxygen Therapy (HBOT) improves oxygenation and inhibits anaerobes. IV Immunoglobulin (IVIG) helps neutralize streptococcal superantigen toxins in toxic shock syndrome.
Fournier's Gangrene
►Definition
Fournier's gangrene is a fulminant, polymicrobial necrotising fasciitis of the perineal, perianal, and genital regions. It is a true surgical emergency characterised by rapid tissue destruction and severe sepsis.
Etiopathology
- Sources of Infection:
- Anorectal (30–50%): Perianal abscess, rectal perforation, haemorrhoidal injections, fissure.
- Urogenital (20–40%): Urethral stricture, periurethral abscess, extravasation of urine, chronic catheterisation.
- Cutaneous: Boils, scrotal trauma, poor hygiene, insect bites.
- Microbiology: Polymicrobial and synergistic. Common isolates include Escherichia coli, Bacteroides fragilis, Streptococcus, Staphylococcus, Pseudomonas, and Clostridium.
- Risk Factors: Diabetes mellitus (most common, present in up to 70%), chronic alcoholism, malnutrition, obesity, HIV, and immunosuppressive therapies.
Pathophysiology
Clinical Features
- Scrotal/perineal pruritus, swelling, pain, and erythema.
- Rapid progression to scrotal swelling, dusky discoloration, tense bullae, crepitus, and frank gangrene.
- Foul-smelling, putrid discharge.
- Severe systemic features: High fever, chills, tachypnea, altered sensorium, and septic shock.
Management Strategy (Immediate vs. Subsequent)
1. Immediate Management (Emergency Stabilization)
-
Resuscitation & Correction:Aggressive crystalloid fluid resuscitation, correction of electrolyte imbalances (hyponatremia is common), and intensive care monitoring.
-
Broad-Spectrum Antibiotics:Start immediately: Meropenem (or Piperacillin-Tazobactam) + Clindamycin + Vancomycin. Adjust based on culture results.
-
Urgent Radical Surgical Debridement:Immediate surgical excision of all necrotic, non-viable skin, subcutaneous tissue, and fascia. Expose healthy, bleeding margins. Do not delay surgery for imaging.
-
Urinary & Fecal Diversion:Place a Foley catheter. Perform a suprapubic cystostomy (SPC) if the urethra is compromised or catheterization is impossible. A defunctioning loop colostomy is required if there is extensive perianal gangrene or active sphincter involvement to prevent continuous faecal contamination of the perineal wound.
2. Subsequent Management (Wound Care & Reconstruction)
-
Repeated Debridements:Schedule planned second-look debridements every 24–48 hours until all necrotic activity has ceased.
-
Negative Pressure Wound Therapy (NPWT/VAC):Apply vacuum-assisted closure once the wound is clean and free of active infection to accelerate granulation tissue formation.
-
Testicular Preservation:The testes are usually spared because they have a separate blood supply (testicular artery directly from the abdominal aorta) and are protected by the tunica vaginalis. They can be temporarily tucked into subcutaneous pockets in the thigh (thigh pouches) to keep them viable and moist.
-
Reconstruction:Once the wound is clean and granulating, perform split-thickness skin grafting (STSG) or scrotal reconstruction using local skin or fasciocutaneous advancement flaps.
Intra-abdominal Abscess
►Definition
An intra-abdominal abscess is a localised collection of pus within the peritoneal cavity or retroperitoneal space, walled off by the omentum, inflammatory adhesions, or adjacent viscera. It typically occurs as a complication of peritonitis, hollow viscus perforation, or post-abdominal surgery.
Classification
| Classification Basis | Type | Definition / Etiology | Examples / Clinical Significance |
|---|---|---|---|
| Etiology | Primary intra-abdominal abscess | Develops after established intra-abdominal infection that ruptures into peritoneal cavity and gets walled off. | Ruptured appendix with localized abscess; perforated diverticulitis with abscess. Common in acute surgical emergencies. |
| Delayed primary intra-abdominal abscess | Initially sterile leak → later bacterial colonization → abscess formation. | Anastomotic leak → pelvic abscess; subphrenic abscess post-cholecystectomy; leak from infected bile post-cholecystitis. Presents days–weeks post-surgery. | |
| Secondary intra-abdominal abscess | Abscess formation in a previously sterile fluid collection due to secondary infection. | Pancreatic pseudocyst → infected; infected sterile ascites; infection via drains/instrumentation. Common in post-operative or debilitated patients. | |
| Location | Intraperitoneal abscess | Within peritoneal cavity. | Subphrenic, paracolic, interloop abscess. Frequently follows GI perforation. |
| Retroperitoneal abscess | Localized infection behind peritoneum. | Perinephric abscess, psoas abscess. Difficult diagnosis; vague symptoms. | |
| Pelvic abscess | Accumulation in pelvis due to gravity. | Rectouterine pouch (Douglas' abscess), rectovesical pouch. Common after pelvic sepsis or surgery. | |
| Solid organ intraparenchymal abscess | Localized abscess within organ parenchyma. | Liver abscess, splenic abscess. May follow hematogenous spread or local infection. | |
| Risk Status | Low risk | Small, well-localized, stable patient. | Small post-appendicectomy abscess. Sometimes conservative management possible. |
| Moderate risk | Larger or symptomatic abscess, moderate sepsis. | Pelvic abscess with fever. Usually requires percutaneous drainage. | |
| High risk | Large, multiple, associated with severe sepsis, poor host factors. | Multiloculated abscess, ruptured viscus with peritonitis → abscess. Urgent drainage (surgical/percutaneous) + antibiotics. |
Clinical Features
- Swinging high-grade fever with chills and rigors.
- Persistent localized abdominal pain and tenderness.
- Anorexia, weight loss, and leucocytosis.
- Site-Specific Signs:
- Subphrenic: Shoulder tip pain (due to phrenic nerve irritation), hiccoughs, pleural effusion, and basal atelectasis.
- Pelvic: Diarrhoea, tenesmus, mucus discharge, urinary frequency, and a boggy, tender mass felt on digital rectal/vaginal examination.
- Psoas: Pain on hip extension, hip flexion deformity (psoas sign), and a groin mass.
Investigations
- CT Scan of Abdomen (Gold Standard): Shows a well-defined, round or oval fluid collection with thick, contrast-enhancing rim ("ring-enhancing lesion"), and gas-fluid levels within. Assesses accessibility.
- Ultrasound: Highly useful for subphrenic, pelvic, and liver abscesses; acts as a guide for drainage.
Management
-
Antibiotic Therapy:Start empiric broad-spectrum antibiotics covering Gram-negatives and anaerobes (e.g., Piperacillin-Tazobactam or Ceftriaxone + Metronidazole). Modify based on culture results.
-
Percutaneous Catheter Drainage (PCD) — First Line:USG- or CT-guided placement of a pig-tail catheter. Highly successful for unilocular, accessible abscesses without internal debris or ongoing enteric leak. Contraindicated in bleeding diathesis or if no safe window exists.
-
Surgical Drainage:Indicated for multiloculated abscesses, thick viscous debris (e.g., pancreatic necrosis), failed percutaneous drainage, or when the abscess is caused by an active anastomotic leak or bowel perforation. Can be done laparoscopically or via open laparotomy.
-
Pelvic Abscess Drainage (Special Route):If the abscess is bulging into the rectum or vagina, it can be drained transrectally or transvaginally. Under anaesthesia, a needle aspirates pus, the tract is dilated, and a drainage tube is inserted. Gravity facilitates drainage.
Clostridioides difficile Colitis
►Definition
Clostridioides difficile (formerly Clostridium difficile) infection (CDI) is an antibiotic-associated inflammatory colitis caused by toxigenic strains of C. difficile. It ranges from mild diarrhoea to severe pseudomembranous colitis, toxic megacolon, bowel perforation, and death.
Etiopathology
- Pathogenesis: Alteration of normal colonic flora by broad-spectrum antibiotics (clindamycin, cephalosporins, fluoroquinolones, ampicillin) → Proliferation of C. difficile (spore-forming Gram-positive obligate anaerobe) → Release of Toxin A (enterotoxin) and Toxin B (cytotoxin) → Mucosal cell death, intense neutrophilic inflammation, and plaque-like pseudomembrane formation (composed of fibrin, mucus, and inflammatory cells).
- Transmission: Fecal-oral route via spores that persist in the hospital environment and resist standard alcohol gels. Hand hygiene with soap and water is mandatory.
Management Guidelines (Staging and Treatment)
| Clinical Definition | Clinical Features | Recommended Treatment | Strength of Evidence |
|---|---|---|---|
| Initial episode — Non-severe | WBC < 15,000 /mm³ AND Creatinine < 1.5 mg/dL | Vancomycin 125 mg PO QID × 10 days OR Fidaxomicin 200 mg PO BID × 10 days. Alt: Metronidazole 500 mg PO TID × 10 days (only if others unavailable). | Strong/High (Vanc/Fidax) Weak/Low (Metro) |
| Initial episode — Severe | WBC ≥ 15,000 /mm³ OR Creatinine ≥ 1.5 mg/dL | Vancomycin 125 mg PO QID × 10 days OR Fidaxomicin 200 mg PO BID × 10 days. | Strong/High |
| Initial episode — Fulminant | Hypotension/shock, ileus, or toxic megacolon | Vancomycin 500 mg PO or via NG tube QID + IV Metronidazole 500 mg q8h. If ileus, consider rectal Vancomycin. | Strong/Moderate |
| First recurrence | Recurrence after initial therapy | If initial was Metronidazole → Vancomycin 125 mg PO QID × 10 days. If initial was Vancomycin → Tapered/pulsed Vancomycin regimen (125 mg QID × 10–14 days → BID 1 week → daily 1 week → q2–3d for 2–8 weeks) OR Fidaxomicin 200 mg PO BID × 10 days. |
Weak/Low — Moderate |
| Second or subsequent recurrence | Multiple relapses | Vancomycin in tapered/pulsed regimen OR Fidaxomicin 200 mg PO BID × 10 days OR Vancomycin × 10 days followed by Rifaximin 400 mg PO TID × 20 days. Fecal Microbiota Transplantation (FMT) is recommended. | FMT: Strong/Moderate Others: Weak/Low |
Surgical Intervention
Indicated for toxic megacolon, colonic perforation, or clinical deterioration despite maximal medical therapy. Procedure of choice: Subtotal colectomy with end ileostomy (diverts faeces and resecting the diseased colon).
MRSA Infections & Control
►Definition
Methicillin-Resistant Staphylococcus aureus (MRSA) refers to strains of S. aureus that are resistant to all beta-lactam antibiotics (penicillins, cephalosporins, carbapenems) due to the acquisition of the mecA gene located on the SCCmec chromosome. This gene encodes an altered penicillin-binding protein, PBP2a, which has a very low affinity for beta-lactams, rendering them ineffective.
Epidemiology & Transmission
- HA-MRSA (Hospital-Acquired): Associated with severe invasive infections (SSIs, pneumonia, line sepsis) in hospitalised patients. Typically multidrug resistant.
- CA-MRSA (Community-Acquired): Spreads in close communities. Causes severe skin/soft tissue infections (furunculosis, necrotising cellulitis) and necrotising pneumonia. Often produces the Panton-Valentine Leukocidin (PVL) cytotoxin.
- Transmission: Primarily via contact with hands of healthcare workers or contaminated surfaces/fomites.
Management
-
Mild Skin/Soft Tissue Infections:Incision and drainage (often curative alone). Oral antibiotics: Trimethoprim-Sulfamethoxazole (TMP-SMX), Clindamycin, Doxycycline, or Linezolid.
-
Severe/Systemic Infections:IV Vancomycin (first-line; requires serum trough level monitoring to avoid nephrotoxicity). Alternatives: Linezolid, Daptomycin, Teicoplanin, or Ceftaroline (a 5th-generation cephalosporin with anti-MRSA activity). Avoid all standard beta-lactams.
-
Decolonisation Protocol (for carriers):Indicated for documented MRSA nasal carriers (healthcare workers or pre-op patients).
- Topical 2% Mupirocin ointment applied to the anterior nares twice daily for 5 days.
- Daily body washing with 4% Chlorhexidine gluconate solution for 5 days.
Infection Control Steps
Tuberculous Cervical Lymphadenitis
►Definition
Tuberculous cervical lymphadenitis (TCL), historically known as scrofula, is the most common form of extrapulmonary tuberculosis. It presents as chronic, painless, matted lymphadenopathy of the cervical nodes, and can progress to cold abscess and sinus formation.
Pathology
- Causative Agent: Mycobacterium tuberculosis (most common) or Mycobacterium bovis (via unpasteurized milk).
- Route: Lymphatic drainage from oral cavity/tonsils, or haematogenous spread from a primary pulmonary focus.
- Stages of Lymphadenitis (Jones and Campbell Classification):
- Stage I: Lymphadenitis: Discrete, firm, mobile, painless lymph nodes.
- Stage II: Matted Nodes: Perinodal spread of inflammation causing nodes to stick together.
- Stage III: Cold Abscess: Central caseating necrosis liquefies, forming a soft, fluctuant, non-tender swelling.
- Stage IV: Collar-stud Abscess: The necrotic node perforates through the deep cervical fascia, forming a superficial fluctuant compartment connected via a narrow neck to the deep nodal abscess.
- Stage V: Sinus/Ulcer: The superficial abscess ruptures through the skin, forming a chronic discharging sinus with undermined edges.
Investigations
- FNAC (First-line): Shows granulomatous lymphadenitis, epithelioid cells, Langhans giant cells, and caseating necrosis. ZN stain shows acid-fast bacilli (AFB) in ~40%.
- GeneXpert (CBNAAT): Rapid nucleic acid amplification test; detects TB DNA and rifampicin resistance within hours. Highly sensitive and specific.
- Biopsy: Excision biopsy is performed only if FNAC is non-diagnostic.
Management
-
Antitubercular Therapy (ATT) — Mainstay:Standard 6-month WHO regimen.
- Intensive Phase (2 months): HRZE (Isoniazid, Rifampicin, Pyrazinamide, Ethambutol).
- Continuation Phase (4 months): HR (Isoniazid, Rifampicin, Ethambutol). Extend if response is delayed.
-
Cold Abscess Management:Never perform a formal incision and drainage. Instead, perform serial needle aspiration through healthy skin (oblique/Z-track technique) to prevent sinus formation.
-
Surgical Excision:Limited role. Reserved for diagnostic biopsy when FNAC fails, excision of a persistent discharging sinus, or residual matted nodes that fail to resolve after a full course of ATT. Radical neck dissection is contraindicated.
Mycetoma (Madura Foot)
►Definition
Mycetoma is a chronic, specific, granulomatous, slowly progressive, and destructive inflammatory disease involving the subcutaneous tissue, skin, and underlying bones, most commonly affecting the foot. It is characterised by a pathognomonic triad: painless subcutaneous mass, multiple discharging sinuses, and a purulent discharge containing grains.
Classification
- Eumycetoma (Fungal): Caused by true fungi. Commonest organism is Madurella mycetomatis. Discharge contains black or yellow grains.
- Actinomycetoma (Bacterial): Caused by filamentous aerobic bacteria (actinomycetes) such as Nocardia brasiliensis, Actinomadura madurae, or Streptomyces somaliensis. Discharge contains white, yellow, or red grains.
Epidemiology & Pathogenesis
Endemic in the "Mycetoma Belt" (between 15°S and 30°N latitudes: Sudan, Somalia, India, Mexico). The infection is acquired via minor skin trauma (thorns, splinters) introducing soil-borne organisms. It is common in agricultural workers who walk barefoot. The disease spreads along tissue and fascial planes, invading muscles and bones, but characteristically spares tendons and nerves until very late (explaining the lack of pain and neurological deficit).
Investigations
- MRI of the Foot: The investigation of choice. It shows the pathognomonic "dot-in-circle" sign (high-signal round areas representing granulomas, containing central low-signal dots representing the bacterial/fungal grains).
- Plain X-ray: Shows soft tissue swelling, periosteal reaction (sun-ray appearance, Codman's triangle), and punched-out osteolytic bone cavities.
- Biopsy & Culture: Deep surgical biopsy of tissue and grains (not superficial swab) is the gold standard to identify the species.
Management
-
Actinomycetoma (Bacterial) — Medical:Highly responsive to antibiotics. The standard is the Welsh Regimen:
- Amikacin (15 mg/kg/day for 21 days) + Co-trimoxazole (twice daily for 5 weeks).
- Repeated in cycles until clinical cure (often 3–5 cycles, up to 1 year).
-
Eumycetoma (Fungal) — Combined:Resistant to medical therapy alone.
- Long-term oral antifungals: Itraconazole (200–400 mg daily) or Ketoconazole for 6–12 months. This localises and shrinks the lesion.
- Followed by wide local surgical excision with margins. Recurrence is high (25–50%) if excision is incomplete.
-
Amputation:Indicated as a lifesaving measure in advanced, refractory disease with extensive bone destruction and secondary bacterial osteomyelitis.
Typhoid Enteric Complications
►Definition
Typhoid fever (enteric fever) is a systemic illness caused by the Gram-negative bacillus Salmonella enterica serovar Typhi. While primarily a medical disease managed with antibiotics, surgeons are called to manage its life-threatening abdominal complications: intestinal perforation and massive haemorrhage.
Pathology
Histopathology reveals characteristic histiocytic proliferation with erythrophagocytosis (macrophages containing phagocytosed red blood cells), which is diagnostic.
Clinical Features of Perforation
- Typically occurs during the 2nd to 3rd week of illness.
- Sudden, severe, generalized abdominal pain (peritonitis).
- Rigidity, guarding, rebound tenderness, and disappearance of liver dullness.
- Toxicity, rapid high step-ladder fever with relative bradycardia (Faget sign).
- Altered bowel habits (constipation or diarrhea with "pea-soup" stools).
Investigations
- Blood Culture: Gold standard in the 1st week (positive in ~90%).
- Widal Test: Measures titers against O (somatic) and H (flagellar) antigens (diagnostic value is limited in endemic areas).
- Cultures: Stool and urine cultures are positive in the 2nd–3rd week.
- Imaging: Erect chest X-ray shows free gas under the diaphragm in perforation.
Management
-
Preoperative Resuscitation:Vigorous IV fluid administration, correction of electrolyte imbalance, and placement of an NG tube. Start broad-spectrum antibiotics: Ceftriaxone + Metronidazole.
-
Emergency Laparotomy:A midline incision is made. The perforation is usually a single, oval-shaped opening on the antimesenteric border of the terminal ileum (within 60 cm of the ileocecal valve).
- Simple Closure: If the patient is stable and the perforation is small (<1 cm), freshen the edges and close it in two layers (transversely to avoid narrowing the lumen).
- Wedge Resection: For medium-sized perforations.
- Segmental Resection & Primary Anastomosis: Indicated if there are multiple perforations, extensive gangrene of the bowel wall, or a large solitary perforation. Only performed if the patient is stable and has no gross peritoneal contamination.
- Loop Ileostomy: If the patient is in severe septic shock, malnourished, or has gross faecal peritonitis. The perforated segment is exteriorised or closed and a proximal stoma is created. This is the safest, life-saving option.
- Side-to-side ileotransverse anastomosis: Done in cases with multiple distal ileal ulcers/perforations.
-
Peritoneal Toilet:Thorough peritoneal lavage with warm normal saline. The skin and subcutaneous tissue are often left open (delayed primary closure) to prevent wound infection.
Intestinal Tuberculosis vs. Typhoid
| Feature | Intestinal Tuberculosis | Typhoid |
|---|---|---|
| Etiology | Mycobacterium tuberculosis | Salmonella enterica serovar Typhi |
| Site | Terminal ileum, ileocaecal junction primarily | Terminal ileum (Peyer's patches) primarily |
| Lesion type | Ulcerative (transverse), hyperplastic (mass) | Longitudinal oval ulcers along antimesenteric border |
| Histology | Caseating granulomas, Langhans' giant cells | Necrosis, erythrophagocytosis, histiocytic proliferation |
| Clinical course | Chronic (constitutional + obstructive symptoms) | Acute (fever, toxicity, perforation/bleeding in 2nd–3rd week) |
| Investigation | Barium follow-through: strictures, high caecum; Laparoscopy + biopsy | Blood/stool culture, Widal test, erect X-ray (free gas) |
| First-line treatment | Antitubercular therapy (ATT) | Antibiotics (ceftriaxone, azithromycin) |
| Surgical principles | Conservative resection (strictureplasty, limited resection) | Emergency closure/resection + peritoneal lavage, stoma if septic |
Amoebiasis & Amoebic Liver Abscess
►Definition
Amoebiasis is an infectious disease caused by the protozoan parasite Entamoeba histolytica, transmitted via the faeco-oral route. It manifests as amoebic colitis (dysentery), amoeboma, or extra-intestinal disease, most commonly amoebic liver abscess (ALA).
Pathology
- Intestinal: Trophozoites invade the colonic mucosa, causing flask-shaped ulcers with narrow necks and wide bases. Chronic, localized inflammation can form a granulomatous mass, called an amoeboma, typically in the caecum.
- Hepatic (ALA): Trophozoites enter the portal circulation and travel to the liver. They cause liquefactive necrosis of hepatocytes, forming an abscess cavity. The pus is characteristically sterile and looks like "anchovy sauce" (chocolate brown, odourless paste).
- Amoebic hepatitis: Microscopic necrosis of liver cells without a gross abscess cavity.
- Location: The right lobe of the liver is involved in 80% of cases, particularly segment VIII, because the superior mesenteric vein drains blood preferentially to the right lobe via the portal vein.
Clinical Features
- Amoebic Colitis: Bloody, mucoid diarrhoea (dysentery), abdominal cramps, tenesmus.
- Amoebic Liver Abscess: High-grade fever with chills, night sweats, weight loss, right upper quadrant (RUQ) pain radiating to the right shoulder tip, tender hepatomegaly, bulging of intercostal spaces, pleural effusion, and basal pneumonitis.
Investigations
- Ultrasound/CT of the Liver: Shows a well-defined hypoechoic round cavity close to the liver capsule, typically solitary.
- Serology: Anti-amoebic antibodies (ELISA, IHA, IIF) are highly sensitive and specific.
- Stool Examination: Shows trophozoites or cysts (low sensitivity in liver abscess).
- Laboratory: Anemia, neutrophilic leukocytosis, and LFT alterations: elevated alkaline phosphatase (ALP), mild transaminitis, and hypoalbuminemia.
- Diagnostic Aspiration: Performed only in doubtful cases. Yields thick, chocolate-brown "anchovy sauce" pus. Trophozoites are located in the active outer wall of the abscess, so they are rarely found in the aspirated fluid.
- Colonoscopy: Shows flask-shaped ulcers with intervening normal mucosa. Biopsy is essential to exclude caecal carcinoma in cases of caecal mass (amoeboma).
Management
-
Medical Therapy (First-line):Highly effective. Give oral/IV Metronidazole (750 mg TID for 7–10 days) or Tinidazole. This must be followed by a luminal amoebicide (e.g., Diloxanide furoate 500 mg TID for 10 days or Paromomycin) to eradicate remaining cysts in the bowel lumen and prevent relapses.
-
Indications for Needle Aspiration:Aspiration under USG guidance is indicated in:
- Imminent rupture (large abscess >5 cm, especially in the left lobe, which can rupture into the pericardium).
- No clinical improvement (fever/pain persisting) after 48–72 hours of appropriate metronidazole therapy.
- Diagnostic uncertainty (to rule out pyogenic abscess or echinococcal cyst).
- Secondary bacterial infection.
-
Surgical Drainage:Reserved for complications: rupture into the peritoneal cavity (causing peritonitis), pleural cavity, or pericardium. Open laparotomy, peritoneal toilet, and drainage are performed.
- Ruptured abscess: Drainage + lavage.
- Toxic megacolon: Bowel resection with exteriorisation.
- Persistent amoeboma: Colonic resection for suspected carcinoma or failure of medical therapy.
Ascariasis Surgical Complications
►Definition
Ascariasis is an infection caused by the giant intestinal roundworm, Ascaris lumbricoides. It affects nearly 25% of the world's population, especially in tropical, humid climates with poor sanitation. It is of major surgical importance due to mechanical complications caused by the migration and bolus formation of adult worms.
Life Cycle & Pathogenesis
The adult worm can grow up to 45 cm. Eggs in the biliary tree may act as a nidus for gallstone formation.
Surgical Complications
- Intestinal Obstruction: Most common complication, especially in children. A large mass (bolus) of tangled worms blocks the terminal ileum. Can lead to pressure necrosis, bowel ischaemia, intussusception, volvulus, and perforation.
- Biliary Ascariasis: Worms migrate through the ampulla of Vater into the common bile duct (CBD), causing biliary colic, ascending cholangitis, cholecystitis, or stricture.
- Pancreatic Ascariasis: Migration into the pancreatic duct causes acute pancreatitis.
- Appendicitis: Worms obstruct the appendiceal lumen, leading to acute appendicitis.
Investigations
- Blood: Eosinophilia.
- Stool Examination: Shows characteristic ova.
- Sputum/Bronchial Washings: May show larvae and Charcot-Leyden crystals during the pulmonary phase.
- Plain Abdominal X-ray: Shows multiple air-fluid levels and a soft tissue mass containing gas bubbles in the RIF (the "whirlpool" or "spaghetti" sign).
- Barium Follow-Through: Shows a bolus of worms or barium within the worm lumen ("double-line" sign).
- Ultrasound: Shows a moving, echogenic, strip-like structure without acoustic shadowing within the CBD ("double-tube" sign).
- MRCP: Detects adult worms in the CBD.
Management
1. Uncomplicated Intestinal Obstruction
Manage conservatively first: NPO, IV fluids, NG suction. Administer hypertonic saline enemas to help paralyze and break up the worm bolus and improve bowel motility. Do not give anthelmintic drugs immediately.
2. Surgical Obstruction
Indicated if conservative management fails, or if there are signs of strangulation/peritonitis.
- Milking: Expose the ileum, gently massage and milk the worm bolus downstream into the caecum/colon (where the lumen is wide).
- Enterotomy: If milking fails, perform a longitudinal enterotomy, extract the worms, and close the bowel.
- Resection & Anastomosis: For bowel necrosis/strangulation.
- Ileostomy: Created in the presence of bowel perforation.
3. Biliary/Pancreatic Ascariasis
Start conservative therapy (antispasmodics, IV fluids). If symptoms persist or cholangitis develops, perform ERCP with endoscopic extraction of the worm using basket/forceps. If ERCP fails, open choledochotomy and surgical extraction are required.
Ascariasis Clinical Stages Summary
| Stage | Manifestations | Investigations | Management |
|---|---|---|---|
| Larval (lung) | Loeffler's syndrome (dry cough, wheeze, dyspnea, fever) | CXR (fleeting infiltrates), eosinophilia, sputum larvae | Symptomatic care only (self-limiting) |
| Adult (intestine) | Abdominal pain, malnutrition, growth retardation | Stool ova | Oral Anthelmintics (Albendazole) |
| Bolus in ileum | Intestinal obstruction, perforation peritonitis, volvulus | AXR (whirlpool sign), barium, CT | Conservative first (hypertonic saline enemas) → Surgery (Milking/Enterotomy) if failed |
| Biliary/Pancreatic | Cholangitis, jaundice, cholecystitis, acute pancreatitis | USG (double-tube sign), MRCP | Conservative → ERCP worm extraction → Surgery (CBD exploration) if failed |
Hydatid Disease of Liver
►
Definition
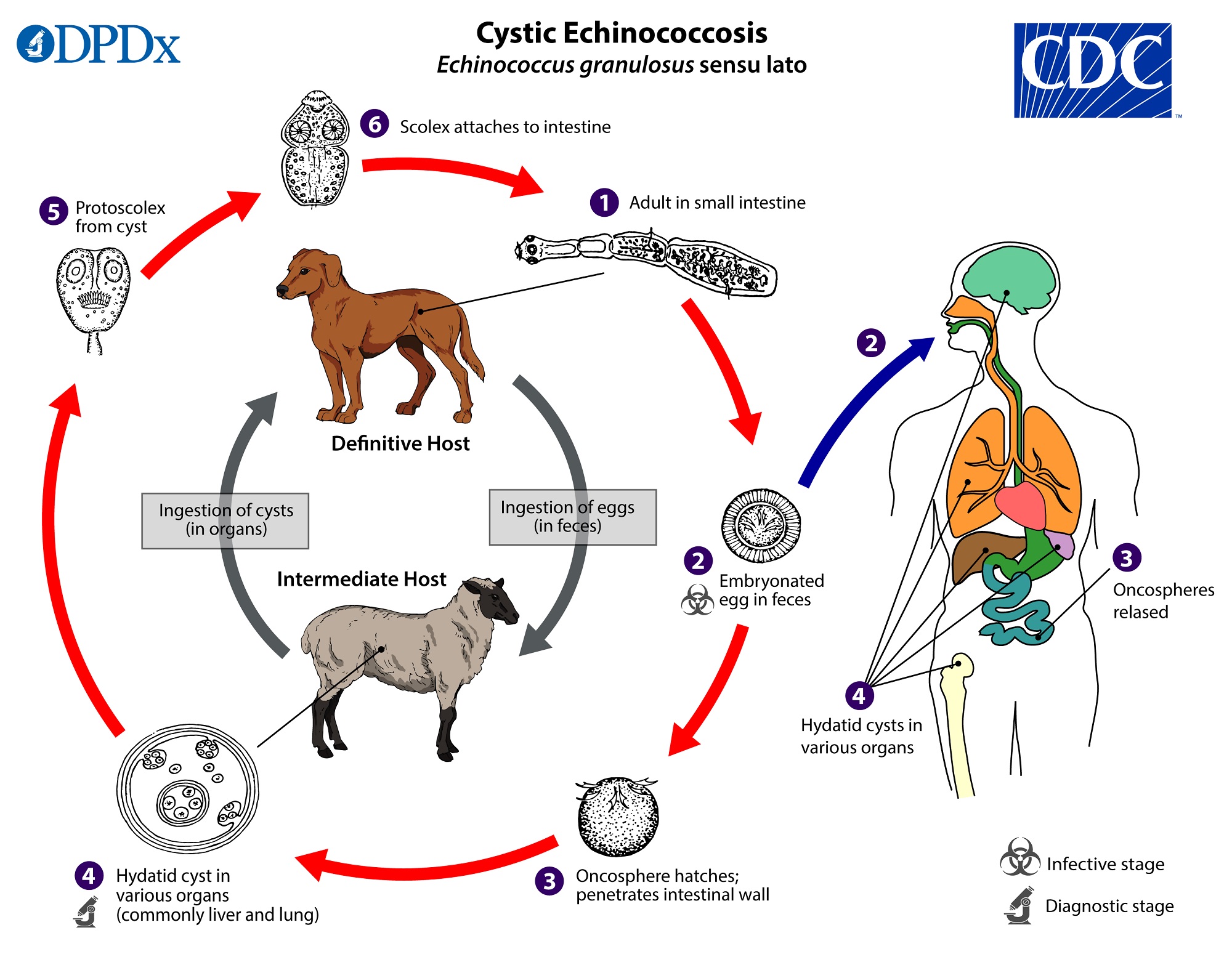
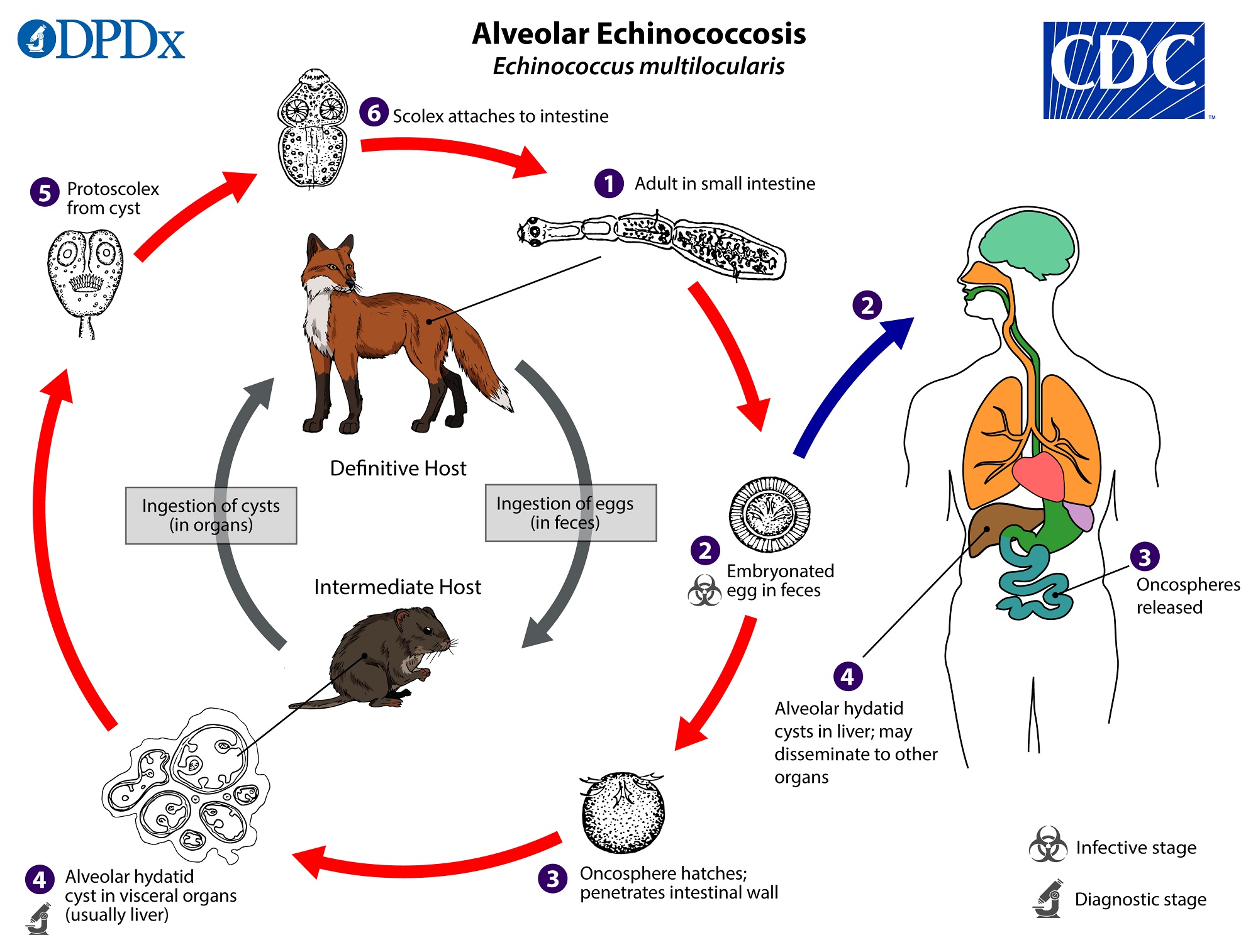
Hydatid disease (Echinococcosis) is a zoonotic parasitic infection caused by the larval stage of the tapeworm Echinococcus granulosus (causing unilocular hydatid cyst) or E. multilocularis (causing alveolar hydatid disease, behaves like a malignant tumor). It is characterised by the formation of slow-growing, fluid-filled cysts in various organs, most commonly the liver (65–70%).
Life Cycle & Cyst Structure
- Hosts: Definitive host: Dog (harbors adult worm in intestine). Intermediate host: Sheep, cattle, goats. Accidental host: Human (dead-end host, acquires infection via ingestion of food/water contaminated with dog faeces containing eggs).
- Cyst Wall Structure:
- Pericyst: Outer fibrous capsule derived from compressed host liver tissue and inflammatory reaction. Vascular.
- Ectocyst: Middle, acellular, gelatinous laminated membrane. Allows nutrient passage.
- Endocyst: Inner, germinal membrane. Produces brood capsules, protoscolices (which break off to form "hydatid sand"), and daughter cysts.
WHO Ultrasound Classification
| Stage | Ultrasound Features | Clinical Status | Management |
|---|---|---|---|
| CE 1 | Unilocular, pure fluid, "snowstorm" sign (hydatid sand) | Active / Fertile | PAIR or Albendazole |
| CE 2 | Multivesicular, daughter cysts, "honeycomb" or "wheel-spoke" pattern | Active / Fertile | Surgery or PAIR (if feasible) |
| CE 3a | Fluid with detached, floating membranes ("water-lily" sign) | Transitional (degenerating) | PAIR or Surgery |
| CE 3b | Solid matrix with daughter cysts | Transitional (degenerating) | Surgery ± Albendazole |
| CE 4 | Heterogeneous solid/fluid mass, "ball of wool" sign | Inactive (dying) | Watch & Wait (observe) |
| CE 5 | Thick, calcified wall (calcified egg-shell appearance) | Inactive (dead) | Watch & Wait (observe) |
Gharbi Classification
- Type I: Pure fluid collection (equivalent to CE1).
- Type II: Fluid with floating membranes (equivalent to CE3a).
- Type III: Septated honeycomb cyst (equivalent to CE2).
- Type IV: Heterogeneous solid/fluid mass (equivalent to CE4).
- Type V: Thick calcified wall (equivalent to CE5).
Medical Management
- Indications: Small active CE1 cysts (<5 cm), multiple or multiorgan cysts, recurrence, cysts in brain, bone, eye, or lung, or inoperable/surgically unfit patients.
- Drugs:
- Albendazole: 10–15 mg/kg/day, in 4-week cycles with a 2-week gap. Mandatory pre-op (1–4 weeks) and post-op (1–3 months).
- Mebendazole: 600 mg/day for 3 months.
- Praziquantel: 60 mg/kg for 2 weeks (synergistic with Albendazole).
- Contraindications: Large cysts, honeycomb/multiseptate cysts, calcified or infected cysts, and pregnancy.
PAIR (Puncture, Aspiration, Injection, Re-aspiration)
- Indications: Inoperable/refuse surgery, CE1–CE3a cysts, relapse cysts, infected cysts, and pregnant women/children.
- Contraindications: Inaccessible cysts, honeycomb/multiseptate cysts, calcified cysts, pulmonary cysts, or cysts communicating with the bile ducts.
- Scolicidal Agents:
Agent Concentration Exposure Time Remarks / Risks Hypertonic saline 15–30% 10 mins Preferred, safest. Risk: Hypernatremia. Alcohol 80–95% 15 mins Risk: Sclerosing cholangitis if biliary communication. Povidone iodine — — Effective. Hydrogen peroxide — — Risk: Air embolism. Cetrimide — 5 mins Shortest exposure. Risk: Metabolic acidosis. Formalin — — Strictly contraindicated (causes caustic cholangitis).
Surgical Management (Gold Standard)
1. Conservative Surgery
- Deroofing & Evacuation: The cyst is opened, contents evacuated, and the cavity washed with hypertonic saline.
- Residual Cavity Management:
- Omentoplasty: Viable omental pedicle placed in the cavity and fixed with absorbable sutures (preferred method).
- Capitonage: Infolding the cyst wall with interrupted or spiral sutures from the depth outwards. Difficult in calcified cysts.
- Introflexion: Infolding the edge inward with bites through overlying liver.
- Capitonage: Infolding the cyst wall.
2. Radical Surgery
- Pericystectomy (Closed or Open): Complete excision of the cyst along with the pericyst (host capsule). Closed is removing without opening the cyst; open is opening first. Dissection is performed in the subadventitial plane.
- Near-Total Pericystectomy: If the cyst is adherent to the IVC or major hepatic veins, the adherent portion is sterilized and left behind while the rest is excised.
- Hepatic Resection: Segmentectomy or hemihepatectomy if a lobe is destroyed or vascular-biliary structures are involved.
Technique of Pericystectomy (14 Steps)
-
Preoperative prophylaxis:Administer Albendazole 10–14 mg/kg/day for 4 weeks to sterilize the cyst content.
-
Laparotomy:Perform a subcostal incision, extending to the left if needed.
-
Exploration:Explore the abdominal cavity for any extrahepatic hydatid disease.
-
Field Protection:Pack the operative field with mops soaked in 20% hypertonic saline (scolicidal agent) to catch any spillage.
-
Intraoperative USG:Assess the relationship of the cyst to the hepatic veins and inferior vena cava (IVC).
-
Hemostasis Control:Maintain low Central Venous Pressure (CVP < 5 mm Hg) to minimize parenchymal bleeding.
-
Inflow Control:Tape the hepatoduodenal ligament for a Pringle maneuver if major bleeding occurs.
-
Traction:Place stay sutures around the cyst wall for traction.
-
Capsule Incision:Incise the liver capsule over the cyst with diathermy.
-
Plane Identification:Identify the correct avascular subadventitial plane between the exocyst and pericyst.
-
Dissection:Dissect the liver parenchyma around the cyst using Kelly clamps or ultrasonic energy devices.
-
Radicle Ligation:Systematically identify, ligate, and underrun any crossing biliary radicles and blood vessels.
-
Abandonment Rule:If the dissection becomes extremely difficult near major vessels, abandon pericystectomy and perform deroofing + evacuation.
-
Cavity Inspection & Wash:Inspect the raw cavity, suture any visible leaks, wash thoroughly, and perform omentoplasty.
Management of Cystobiliary Communications (CBC)
- Identification: Bile-stained cyst fluid, repeated saline wash to locate leaks, needle injection into the CBD with saline, air, or methylene blue, or intraoperative cholangiography.
- Management:
- Small CBC: Simple suture closure with 4-0 Vicryl/PDS.
- CBC with CBD debris: Choledochotomy, debris removal, choledochoscopy, T-tube drainage, and T-tube cholangiogram.
- Unsuturable CBC: Bipolar drainage (external drainage of the pericyst cavity + T-tube in the CBD) or the Perdomo procedure (multiperforated drain through the fistula tract into the cyst + another drain in the cavity + T-tube in the CBD).
- Major Biliary Duct involvement: Roux-en-Y cystojejunostomy, intracystic hepaticojejunostomy, or liver resection.
Postoperative Complications
| Complication | Common Cause | Management |
|---|---|---|
| Biliary leak | Missed CBC, biliary injury, retained debris, calcified cyst | Conservative first (drain) ± ERCP + sphincterotomy |
| Infection / Sepsis | Infected residual cavity | Antibiotics + image-guided percutaneous drainage |
| Subphrenic abscess | Postoperative fluid accumulation/infection | Percutaneous drainage + IV antibiotics |
| Liver failure | Extensive hepatectomy on compromised liver | Supportive care (high mortality) |
| Recurrence | Retained scolices, incomplete evacuation, spillage | Secondary hydatids; repeat surgery or long-term Albendazole |
Intestinal Tuberculosis
►Definition
Intestinal tuberculosis is a chronic granulomatous infection of the gastrointestinal tract caused by Mycobacterium tuberculosis or Mycobacterium bovis. It most commonly affects the ileocecal region (85% of cases) due to the abundance of lymphoid tissue (Peyer's patches), physiological stasis, and high absorptive capacity in this area.
Pathological Types
| Pathological Type | Morphology & Histology | Clinical Presentation |
|---|---|---|
| Ulcerative Type | Multiple transverse (circular) ulcers with undermined edges. Caused by high bacillary virulence in patients with low immunity. Histology shows caseating granulomas with Langhans' giant cells. Healing leads to fibrosis and circular strictures. | Presents with chronic intestinal obstruction (subacute/acute) due to multiple strictures. Perforation is rare. |
| Hyperplastic Type | Marked inflammatory hyperplasia and thickening of the caecal and ileal walls, mimicking Crohn's disease. Host immunity is high. Fibrosis pulls the caecum upward into the subhepatic region, widening the ileocaecal angle. | Presents as a painless, firm mass in the right iliac fossa (RIF), causing subacute obstruction. |
| Peritoneal / Ascitic | Peritoneum studded with tubercles. Loculated ascites, "doughy" feel of abdomen, and fibrotic cocoon formation. | Ascites, distension, abdominal pain. |
Clinical Features
- Constitutional symptoms: Low-grade evening fever, night sweats, weight loss, anorexia.
- Chronic abdominal pain, distension, alternating diarrhoea and constipation.
- Physical Exam: Palpable mass in the RIF (hyperplastic type), "doughy" feel of the abdomen (peritoneal ascites), or multiple perianal fistulae with undermined edges.
- Acute Presentation: Acute/subacute intestinal obstruction due to strictures, or peritonitis from perforation of a tuberculous ulcer (rare).
Investigations
- Barium Meal Follow-Through (Classic): Shows multiple strictures in the terminal ileum, a "high subhepatic caecum" (pulled up by fibrosis), a straight ileocecal junction, or the "Stierlin sign" (rapid emptying of the inflamed caecum leaving a narrow barium column).
- CT Abdomen: Shows mural thickening of the ileocaecal region, necrotic mesenteric lymphadenopathy, ascites, and cocoon formation.
- Endoscopy & Biopsy: Shows mucosal ulcers or nodules. Biopsy shows caseating granulomas (differentiates it from non-caseating granulomas of Crohn's disease).
- Diagnostic Laparoscopy: Direct visualization of tubercles, strictures, lymph nodes, and ascites; biopsy is gold standard.
Management
-
Medical Treatment (First-line):Mainstay of therapy. Standard anti-tubercular therapy (ATT) regimen under DOTS for 6 months (2 months HRZE + 4 months HR, extending to 9 months in complicated cases). Ensure aggressive nutritional support.
-
Strictureplasty (Bowel-Sparing Surgery):The surgical procedure of choice for short, segment-specific strictures causing obstruction. The stricture is incised longitudinally and closed transversely (Heineke-Mikulicz technique) to widen the lumen without resecting bowel. Conserves bowel length and prevents malabsorption.
-
Limited Resections:
- Limited Ileocolectomy: Resection of the diseased terminal ileum and caecum with primary anastomosis, indicated for localized hyperplastic caecal mass.
- Segmental Resection: Resection of a segment for multiple closely placed strictures.
- Right Hemicolectomy: Reserved for extensive caecal involvement with multiple proximal strictures.
-
Emergency Management:If the patient presents with acute perforation peritonitis or complete obstruction, they are often severely malnourished and toxic. Perform resection of the diseased segment and create a proximal loop ileostomy and distal mucus fistula. Avoid primary anastomosis in unstable, septic patients as the anastomotic leak rate is extremely high. Perforation is handled with segmental resection + stoma.
| Feature | Intestinal Tuberculosis | Crohn's Disease |
|---|---|---|
| Ulcers | Transverse (circular) | Longitudinal, aphthous, cobblestone |
| Granulomas | Caseating (necrotic), large, multiple | Non-caseating, small, discrete |
| Lymph Nodes | Matted, caseous necrosis | Discrete, reactive, no caseation |
| Fistulae | Rare | Common (entero-cutaneous, entero-enteric) |
| Treatment | Antitubercular Drugs (ATT) | Immunosuppressants / Steroids (ATT makes Crohn's worse; Steroids make TB fatal) |
Sources & References
- Bailey & Love's Short Practice of Surgery (28th Edition)
- Sabiston Textbook of Surgery (21st Edition)
- Recent Advances in Surgery