Minimal Access & Robotic Surgery
From the 9 core principles of MAS and SILS cosmesis to the 7-degree EndoWrist, AR overlays and AI decision support — the complete technology landscape of modern minimally invasive surgery.
Minimal Access Surgery — Principles
►
Definition
Minimal Access Surgery (MAS) refers to surgical techniques performed through small incisions or natural orifices, using specialised instruments and imaging systems, to reduce operative trauma while achieving outcomes comparable to conventional open surgery.
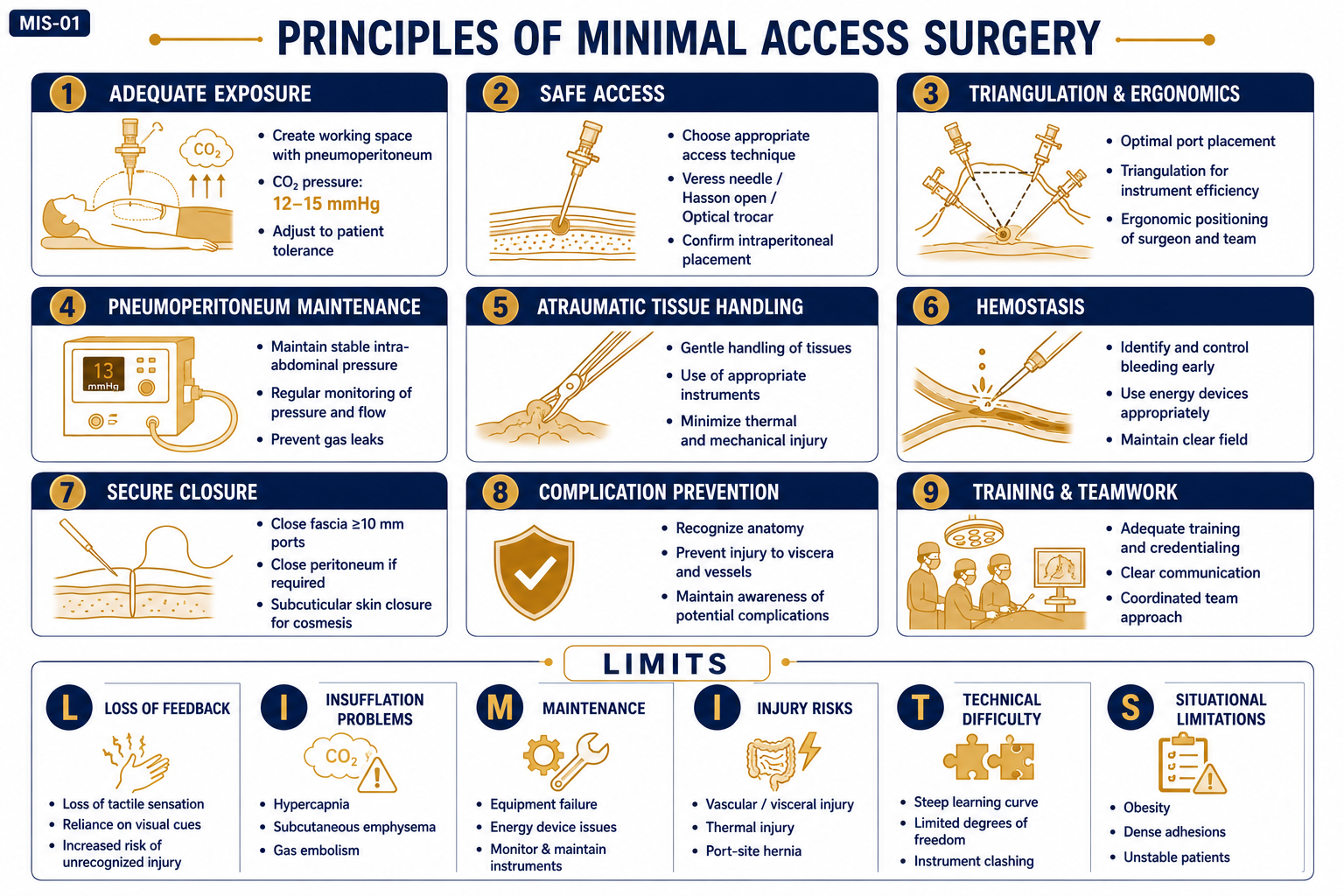
9 Core Principles of MAS
1. Adequate Exposure & Visualisation
- Achieved by pneumoperitoneum (CO&sub2; insufflation, 12–15 mmHg) or mechanical retraction (gasless techniques)
- Requires high-definition endoscopic camera with magnification
2. Safe Access to Body Cavities
- Entry techniques: Closed (Veress needle), Open (Hasson technique), Optical trocar entry
- Proper placement of primary and secondary ports under vision is essential
3. Triangulation & Ergonomics
- Instruments and camera ports positioned to form a working triangle for optimal manoeuvrability
- Avoid “sword fighting” of instruments (crossing of instrument shafts)
4. Maintenance of Pneumoperitoneum
- Safe intra-abdominal pressure: 12–15 mmHg (lower in children and cardiopulmonary compromise)
- CO&sub2; preferred: rapidly absorbed, non-flammable, inert
5. Atraumatic Tissue Handling
- Atraumatic graspers; minimal cautery; avoidance of unnecessary traction
- Respect for tissue planes; minimal desiccation
6. Haemostasis
- Energy sources: monopolar, bipolar, harmonic scalpel, vessel sealing devices
- Secure control of major vessels before division
7. Secure Closure of Visceral Defects
- Intracorporeal or extracorporeal suturing, staplers, or clips
- Port sites ≥10 mm must be closed to prevent port-site hernia
8. Prevention of Complications
- Proper patient positioning (Trendelenburg, reverse Trendelenburg, lithotomy)
- Avoid hypothermia, hypercarbia, air embolism
- Continuous cardiopulmonary monitoring
9. Adequate Training & Teamwork
- Steep learning curve; requires skilled surgeon, assistant, and trained OT team
- Simulation and modular training programmes improve safety
Advantages of MAS
- Reduced postoperative pain
- Shorter hospital stay and faster recovery
- Smaller scars; better cosmesis
- Reduced wound complications and infection
- Magnified operative field — improved visualisation of structures
Limitations — Mnemonic “LIMITS”
| Letter | Limitation | Detail |
|---|---|---|
| L | Loss of tactile feedback | No palpation; reduced haptic sense |
| I | Insufflation-related problems | CO&sub2; absorption → acidosis, ↓ venous return, gas embolism |
| M | Maintenance issues | Costly equipment; need for servicing; availability in low-resource settings |
| I | Injury risks | Trocar, vascular, visceral injuries; port-site hernia; port-site metastasis |
| T | Technical difficulty & learning curve | 2D view; rigid instruments; steep skill acquisition |
| S | Situational limitations | Severe adhesions, pregnancy, sepsis, cardiopulmonary compromise |
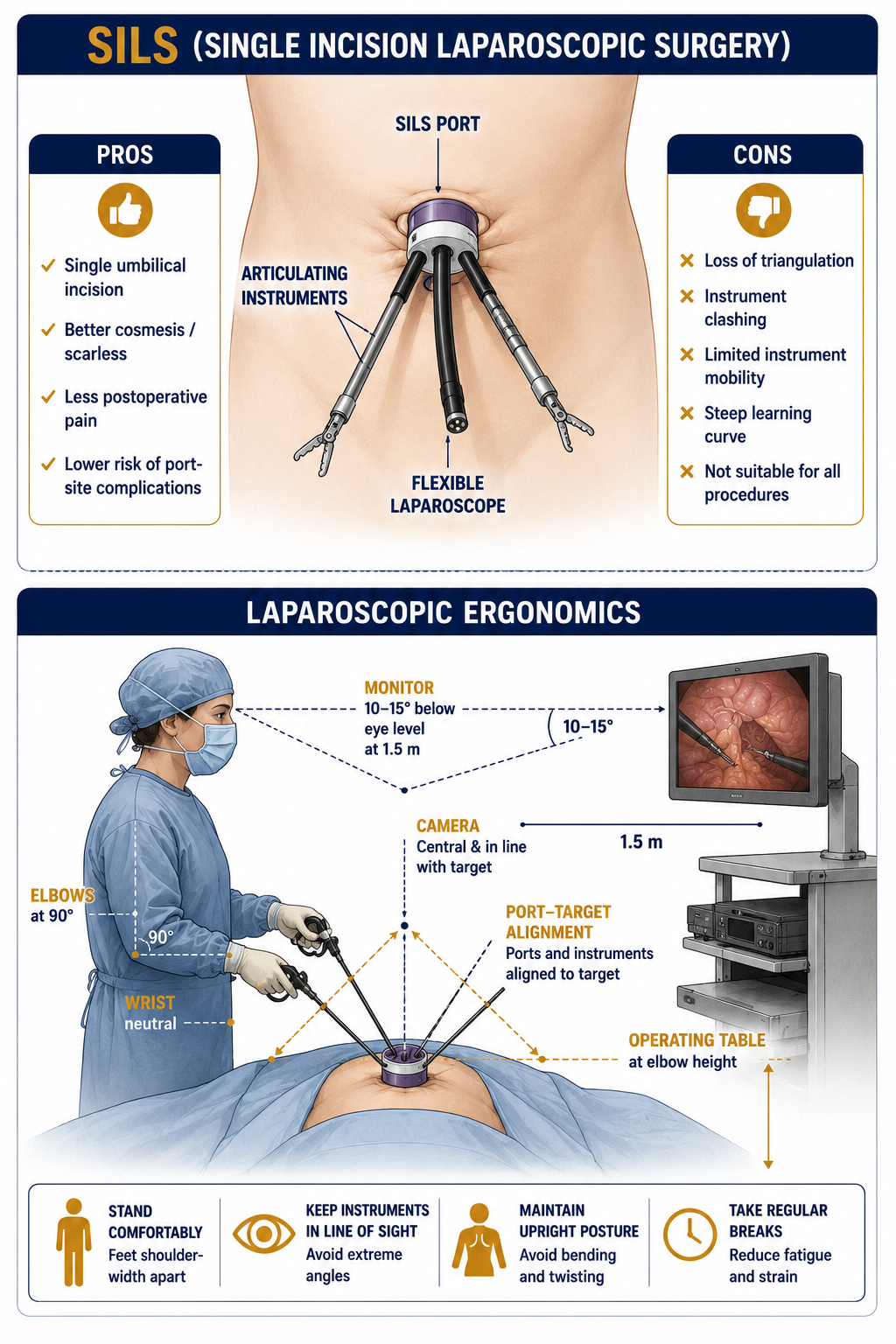
Single Incision Laparoscopic Surgery (SILS)
►
Definition
SILS is a minimally invasive surgical technique where all instruments and the laparoscope are inserted through a single umbilical incision, instead of multiple ports as in conventional laparoscopy. It utilises the natural scar of the umbilicus to minimise visible scarring.
Equipment Required
- Special SILS port (multi-channel; e.g., SILS Port, GelPOINT)
- Articulating or curved/prebent instruments (to avoid clashing)
- Flexible laparoscope (30° or 45°) or roticulating camera
Advantages
- Better cosmesis — near-scarless result (scar hidden in umbilicus)
- Less postoperative pain
- Faster recovery and earlier discharge
- Reduced port-site complications (infection, hernia, bleeding)
Disadvantages / Limitations
- Loss of triangulation → reduced instrument manoeuvrability
- Instrument crowding & clashing (“chopstick effect”)
- Steep learning curve; longer operative time initially
- Limited indications; not suitable for complex cases
Common Indications
- Cholecystectomy (most common SILS procedure)
- Appendectomy
- Nephrectomy (simple)
- Selected bariatric procedures
- Gynaecological surgeries (oophorectomy, tubal ligation)
Contraindications
- Extensive intraperitoneal adhesions
- Obese or unfit patients
- Complicated cases (perforation, malignancy requiring wide resection)
Recent Advances in SILS
- Robotic SILS: Robotic platform improves dexterity and instrument triangulation within a single port
- NOTES hybrid techniques: Combining single incision with natural orifice access
Mnemonic “SILS”
- S — Single umbilical port
- I — Improved cosmesis
- L — Limited triangulation
- S — Special instruments required
Ergonomics in Laparoscopic Surgery
►Definition
Ergonomics in laparoscopic surgery refers to the scientific design of instruments, operating room layout, and surgeon posture to ensure maximum efficiency, precision, and comfort, while minimising fatigue, strain, and musculoskeletal injury.
Core concept: “Fit the surgery to the surgeon.”
Ideal Ergonomic Standards
| Aspect | Ideal Ergonomic Standard |
|---|---|
| Surgeon posture | Upright, relaxed shoulders, elbows at 90°, wrists neutral |
| Monitor position | Directly in front, 10–15° below eye level, at ~1.5 m distance |
| Table height | At or slightly below elbow level |
| Port placement | In line with target organ; comfortable hand angles 30–45° |
| Instrument length | 30–45 cm for optimal internal reach and external ergonomics |
| Camera position | Perpendicular to operative field (camera–target–instrument alignment) |
| Foot pedals | Within natural reach; stable placement |
Common Ergonomic Problems & Solutions
| Problem | Solution |
|---|---|
| Neck & shoulder pain (high monitor / awkward posture) | Proper monitor alignment; adjustable height table |
| Hand & wrist strain (poorly designed instruments) | Ergonomically curved instruments with thumb-neutral grips |
| Back pain (prolonged static posture) | Alternate standing/sitting; maintain balanced stance |
| Eye strain (prolonged 2D focus, poor monitor angle) | High-resolution 3D monitors; frequent visual breaks |
| General fatigue | Anti-fatigue mats; optimise team task rotation |
Ideal Ergonomic Instrument Features
- Lightweight, balanced handle
- Neutral wrist alignment (in-line axis)
- Handle–shaft angle ~100–120°
- Low actuation force
- Rotatable and insulated shafts
Benefits of Good Ergonomics
- Reduced surgeon fatigue and musculoskeletal injury risk
- Improved precision, stability, and operative efficiency
- Fewer technical errors and lower conversion rates
- Enhanced career longevity and surgeon well-being
Robotic Surgery
►
Types of Surgical Robots
| Type | Mechanism | Example |
|---|---|---|
| Supervisory-controlled (Autonomous) | Robot performs pre-programmed tasks autonomously | ROBODOC (orthopaedic bone milling), Neuromate |
| Tele-surgical (Master–Slave) | Surgeon operates from console; robot mimics movements in real time | da Vinci Surgical System |
| Shared-control (Co-manipulation) | Surgeon and robot work together; robot filters tremor | Used in neurosurgery, microvascular surgery |
| Autonomous / AI-assisted | Robot performs specific tasks with AI; limited human input | Experimental — AI-driven tissue dissection, suturing robots |
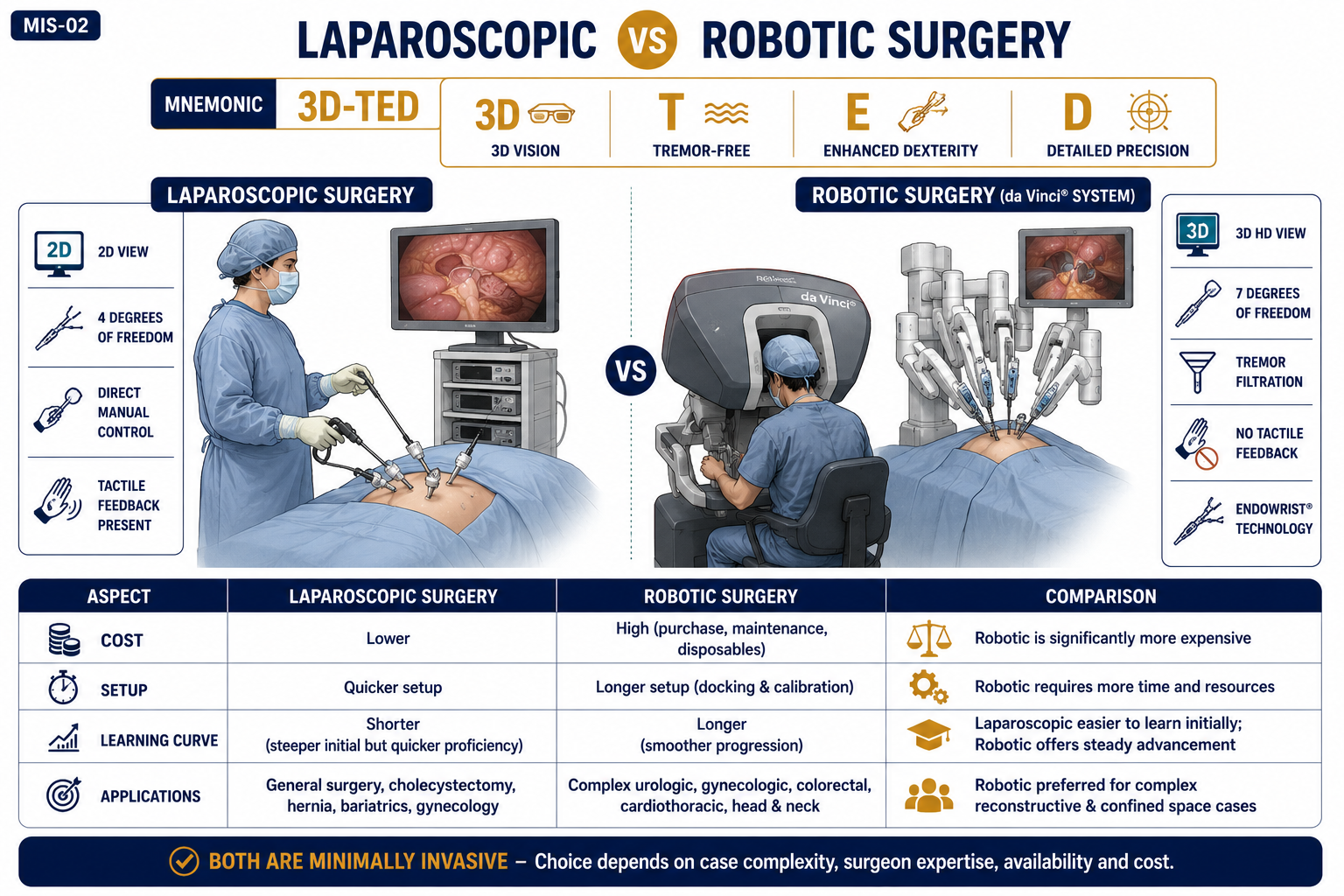
Laparoscopic vs Robotic Surgery — Comparison
| Feature | Laparoscopic | Robotic |
|---|---|---|
| Visualisation | 2D camera view | High-definition 3D magnified view |
| Instrument control | Hand-held rigid instruments | Computer-assisted articulated instruments (EndoWrist) |
| Degrees of freedom | 4 (limited by rigid instruments) | 7 — mimics human wrist movement |
| Tremor filtration | None — manual movement transmitted directly | Yes — electronic tremor elimination |
| Tactile (haptic) feedback | Minimal tactile sensation | Absent (no haptic feedback) |
| Ergonomics | Surgeon stands; may develop fatigue | Surgeon sits at console — ergonomic comfort |
| Setup time | Quick setup | Longer setup & docking time |
| Learning curve | Shorter | Steeper; requires special training |
| Cost | Relatively low | Very high (system + maintenance) |
| Space requirement | Standard OT | Large OT space needed |
| Applications | Routine MIS (lap chole, appendectomy) | Complex confined spaces — prostate, pelvis, cardiac |
| Conversion rate | Slightly higher | Lower conversion rate |
Advantages of Robotic over Laparoscopic — Mnemonic “3D-TED”
- 3D — 3D high-definition vision
- T — Tremor-free operation
- E — Enhanced dexterity (7 degrees of freedom)
- D — Detailed precision in confined spaces
Limitations of Robotic Surgery
| Aspect | Limitation |
|---|---|
| Cost | High initial purchase and maintenance cost; consumables expensive |
| Setup time | Longer docking and preparation time |
| Tactile feedback | Absence of haptic sensation — risk of inadvertent tissue injury |
| Space | Requires large operating room |
| Learning curve | Steep training requirements; credentialing needed |
| Availability | Limited to tertiary centres; not widely available in India |
Common Surgical Applications
- Urology: Radical prostatectomy (most common worldwide), pyeloplasty, partial nephrectomy
- Gynaecology: Hysterectomy, myomectomy
- General Surgery: Cholecystectomy, colorectal resections, Heller myotomy
- Thoracic & Cardiac: Mitral valve repair, lobectomy
Augmented Reality & Surgeons
►Definition
Augmented Reality (AR) is a technology that overlays digital information — 3D anatomical models, imaging data, or intraoperative guidance — onto the real-world surgical field in real time, enhancing the surgeon’s perception without removing focus from the operative site.
Principle
AR integrates virtual data (CT, MRI, or ultrasound images) with real-time visualisation of the operative field using specialised head-mounted displays (HMDs), tablets, or projection systems. This requires:
- Image registration: Aligning virtual images with real anatomy
- Tracking systems: Optical or electromagnetic sensors to maintain spatial accuracy
- Display systems: Smart glasses (e.g., Microsoft HoloLens), operating microscopes, or monitors
Applications in Surgery
| Application Area | AR Use |
|---|---|
| Preoperative planning | 3D reconstruction of complex anatomy; simulation of surgical steps; proximity to vital structures |
| Intraoperative navigation | Real-time overlay of imaging onto operative field; tumour, vessel, and duct localisation in MIS/robotic surgery |
| Education & training | Immersive learning environments; practice on virtual patients; objective skill assessment metrics |
| Neurosurgery | Tumour localisation; trajectory planning; avoiding eloquent cortex |
| Hepatobiliary surgery | 3D vascular and biliary mapping; safe resection margins |
| Orthopaedic surgery | Joint replacement alignment; fracture fixation |
| Plastic & reconstructive | Flap design and perfusion assessment |
| ENT & Head–Neck | Navigation around vital neurovascular structures |
Advantages
- Enhanced spatial orientation and depth perception
- Reduces operative time and complications
- Improves accuracy in tumour margin delineation and screw placement
- Promotes surgeon education and patient-specific planning
Limitations
- Registration errors and tracking inaccuracies may mislead navigation
- Latency (time lag) in image update can affect precision
- High cost and need for technical expertise
- User discomfort with prolonged use of head-mounted devices
- Integration with sterile workflow remains a challenge
Mixed Reality (MR)
Combines AR and Virtual Reality (VR), allowing direct interaction with virtual elements overlaid on the real world. Example: Microsoft HoloLens in surgical planning — surgeon can “reach into” the holographic anatomy.
Recent Advances
- AI integration for automatic image segmentation in AR displays
- Haptic feedback systems for tactile realism in AR training
- AR-assisted robotic platforms (da Vinci with AR overlays)
Artificial Intelligence in Surgery
►Definition
Artificial Intelligence (AI) in surgery refers to the use of computer algorithms that mimic human cognition — learning, reasoning, and decision-making — to assist surgeons in diagnosis, planning, intraoperative guidance, and postoperative care.
Core concept: AI uses data + algorithms to provide decision support and automation, improving accuracy, safety, and efficiency.
Types of AI Used in Surgery
| Type | Function | Surgical Example |
|---|---|---|
| Machine Learning (ML) | Learns patterns from data to predict outcomes | Predict post-op complications from preop parameters |
| Deep Learning (DL) | Image-based recognition using neural networks | Tumour detection on CT/MRI; polyp detection at colonoscopy |
| Computer Vision | Identifies structures in operative field | Instrument tracking and phase recognition in laparoscopy |
| Natural Language Processing (NLP) | Extracts and processes clinical notes | Automated operative reports; structured data extraction |
| Robotic AI | Assists precision movements | Autonomous robotic suturing (experimental) |
Applications by Surgical Stage
| Stage | AI Applications |
|---|---|
| Preoperative | Diagnosis, surgical planning, risk prediction, 3D modelling from CT/MRI |
| Intraoperative | Image-guided navigation, robotic assistance, fluorescence mapping, real-time anatomy recognition |
| Postoperative | Complication prediction, outcome analysis, remote monitoring |
| Education / Training | Virtual simulation, skill assessment, teleproctoring feedback |
Advantages
- Enhances precision and decision-making
- Reduces human error and operative time
- Enables personalised surgical planning
- Assists in training and skill evaluation (objective metrics)
- Supports telemedicine and remote surgery
Limitations
- Requires large, high-quality datasets for training
- Risk of algorithmic bias or error
- High cost and infrastructure needs
- Legal and ethical concerns (accountability, data privacy)
- Lacks human judgment and empathy
Ethical & Legal Framework (India)
- Governed by NMC & MoHFW digital health policies and IT Act 2000
- AI use must ensure data confidentiality, patient consent, and accountability
- Final responsibility always lies with the surgeon, not the AI system
3D Printing in Surgery
►Definition
3D printing (Additive Manufacturing) is a process of creating physical, three-dimensional models from digital (CT/MRI) data by adding material layer by layer. Used in surgery for planning, custom implants, prosthetics, and education.
Principle — Steps
- Imaging acquisition: CT/MRI scan of the relevant anatomy
- Digital reconstruction: 3D modelling using CAD (Computer-Aided Design) software; STL file format
- Printing: Layer-by-layer creation using materials like resin, titanium, or polymer
- Sterilisation & use: For planning, implantation, or simulation
Common Surgical Applications
| Field | 3D Printing Use |
|---|---|
| Orthopaedics | Patient-specific bone implants, fracture models, joint replacement guides |
| Craniomaxillofacial | Reconstruction plates, mandible models, contour planning for facial surgery |
| Cardiothoracic / Vascular | Aneurysm, valve, and vessel models for simulation and preoperative planning |
| HPB / Oncosurgery | 3D liver and tumour models for resection planning; volumetry |
| Plastic Surgery | Custom prostheses, flap contouring, ear and nose reconstruction models |
| Education / Simulation | Training models for rare or complex anatomy; resident education |
Materials Used
- Polymers / PLA / ABS — models and surgical guides
- Titanium alloys — orthopaedic and craniofacial implants
- Biocompatible resins / ceramics — dental or reconstructive use
Advantages
- Patient-specific precision — customised implants and cutting guides
- Enhances preoperative planning and reduces operative time
- Improves anatomical understanding for complex cases
- Useful in resident training and patient counselling (patient can visualise their anatomy)
Limitations
- High cost and limited availability
- Requires technical expertise and high-quality imaging
- Time-consuming to print and sterilise — not suitable for emergencies
- Regulatory approval needed for implantable devices (CDSCO / FDA)
Legal & Ethical Aspects
- Must comply with Medical Device Regulations (CDSCO in India, FDA in USA)
- Informed consent required for patient-specific implanted models
- Maintain data privacy for CT/MRI-based reconstructions
Future Directions
- Bioprinting: Printing of tissues/organs using living cells (bioinks); under active research for skin, cartilage, vascular grafts
- Integration with AR/VR for enhanced surgical simulation
- On-site hospital 3D printing labs for emergency customisation