Image-Guided & Diagnostic Surgery
From navigation-aided surgery and stereotaxy to ICG fluorescence and EUS — how modern imaging integrates with the operative field to improve precision, safety and oncological outcomes.
Navigation-Aided (Computer-Assisted) Surgery
►
Definition
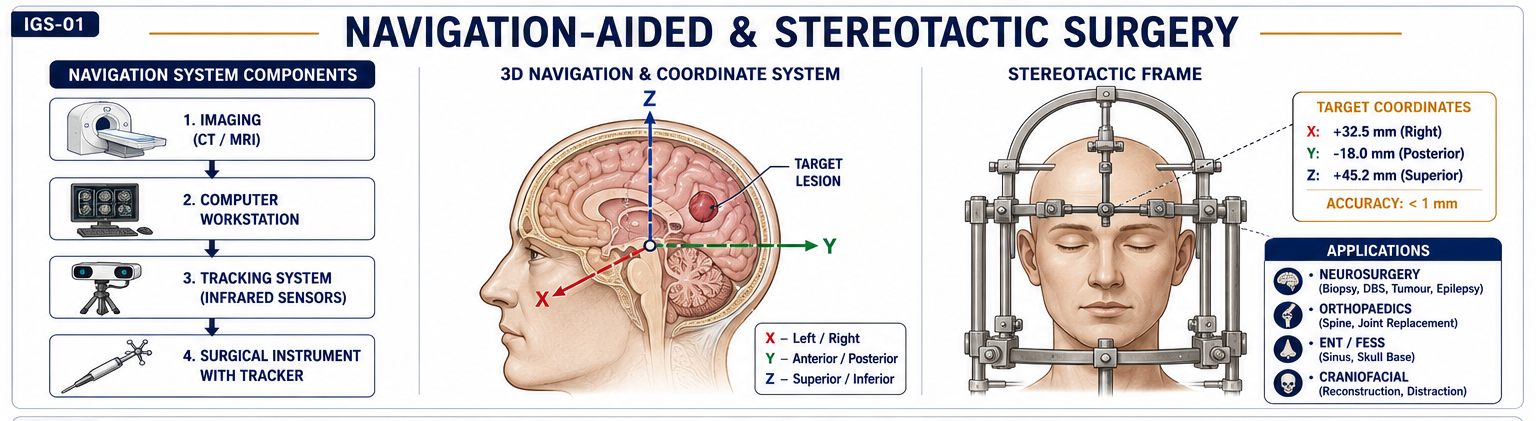
Navigation-Aided or Computer-Assisted Surgery (CAS) uses computer technology and 3D imaging to plan and guide surgical procedures in real time, showing instrument position relative to patient anatomy.
Principle
Combines preoperative imaging (CT/MRI) or intraoperative imaging with tracking systems to provide real-time 3D visualisation. The surgeon can see instrument position overlaid on the patient’s anatomical map at all times.
Components
- Imaging system — CT, MRI, fluoroscopy (preoperative or intraoperative)
- Tracking system — infrared/optical/electromagnetic sensors attached to instruments and patient reference frame
- Computer workstation — registers imaging to patient anatomy; reconstructs 3D model
- Display unit — shows real-time instrument position relative to anatomy on screen
Applications
| Specialty | Application |
|---|---|
| Neurosurgery | Tumour resection, stereotactic biopsy, shunt placement, DBS electrode positioning |
| Orthopaedics | Joint replacement alignment, pedicle screw placement, spinal fixation |
| ENT / Skull base | Functional endoscopic sinus surgery (FESS), skull base tumours |
| Craniofacial / Maxillofacial | Osteotomy planning, implant positioning |
| HPB / Oncosurgery | Tumour localisation, image-guided ablation, margin assessment |
Advantages
- Enhanced accuracy and precision in critical anatomical areas
- Minimally invasive approach possible with greater confidence
- Reduced complications and better outcomes
- Improved surgical planning and intraoperative decision-making
Limitations
- High cost and complex setup; requires dedicated equipment
- Registration errors — mismatch between preoperative image and intraoperative anatomy (brain shift, bowel movement)
- Requires technical expertise and training
- Limited tactile feedback
Stereotactic Surgery
►Definition
Stereotactic (stereotaxic) surgery is a minimally invasive, image-guided surgical technique that uses a 3D coordinate system to accurately localise and target specific areas inside the body for diagnosis or therapy.
Principle
- Combines medical imaging (CT, MRI, PET) with a computer-based coordinate system
- Provides three-dimensional spatial accuracy for instrument navigation
- Defines target using X, Y, Z axes relative to a fixed stereotactic frame or frameless (fiducial-based) system
- Allows accurate guidance of needles, probes, electrodes, or radiation beams to a precise intracranial or body target
Components
- Stereotactic frame (Leksell, CRW) or frameless navigation system
- Imaging — CT/MRI/PET for target localisation
- Computer workstation for planning and coordinate calculation
- Guidance instruments — needle, probe, electrode, radiation beam
Applications
| System / Region | Applications |
|---|---|
| Neurosurgery | Brain biopsy, Deep Brain Stimulation (DBS), Gamma Knife/CyberKnife radiosurgery, functional ablation (tremor, epilepsy) |
| Oncosurgery | Image-guided tumour localisation, biopsy, and radiotherapy planning |
| Orthopaedics | Navigation in spine surgery, joint replacement |
| ENT & Skull base | Navigation-assisted sinus and skull base surgery |
| General Surgery | Liver or lung lesion localisation and ablation |
| Radiation Oncology | Stereotactic radiosurgery (SRS) and radiotherapy (SBRT/SABR) |
| Interventional Radiology | Precise needle placement for biopsy, drainage, ablation |
Advantages
- High precision and reproducibility
- Minimally invasive — reduced morbidity compared to open craniotomy
- Shorter operative time and recovery
- Real-time 3D visualisation in critical anatomical areas
Limitations
- High cost and equipment dependence
- Requires expertise and dedicated imaging support
- Limited use in diffuse or mobile lesions (target must be a discrete, fixed point)
Image Guidance in Surgery (IGS)
►Definition
Image-Guided Surgery (IGS) refers to surgical procedures that use preoperative or intraoperative imaging to localise anatomy, pathology, or instruments in real time, improving accuracy, safety, and outcomes. In short: surgery performed with real-time imaging assistance.
Principle
Combines anatomical imaging (CT, MRI, USG, PET, NIR fluorescence) with computer-assisted navigation systems that track surgical instruments relative to the patient’s anatomy in real time.
System Components
- Imaging source: Preoperative — CT, MRI, PET; Intraoperative — USG, fluoroscopy, ICG-NIR, cone-beam CT
- Navigation system: Optical or electromagnetic trackers for instrument localisation
- Display/Software: 3D reconstruction and real-time overlay of anatomy and instrument position
- Surgeon interface: Monitor, head-mounted display (HMD), or robotic console
Applications by Specialty
| Specialty | IGS Applications |
|---|---|
| Neurosurgery | Stereotactic brain biopsy, tumour resection, shunt placement |
| ENT / Skull Base | FESS, skull base tumour surgery |
| HPB Surgery | Intraoperative USG & ICG mapping for liver resection, biliary mapping |
| Vascular Surgery | Endovascular navigation, fluorescence angiography |
| Orthopaedic Surgery | Pedicle screw placement, joint replacement navigation |
| Oncologic Surgery | Tumour localisation, sentinel node mapping |
| Urology | Partial nephrectomy, prostatectomy with augmented imaging |
| Trauma / Spine | Navigation for fixation and decompression |
Recent Advances in IGS
- Fluorescence-guided surgery (ICG-based) — perfusion and biliary mapping
- Augmented Reality (AR) and Virtual Reality (VR) overlays — projecting 3D anatomy onto the operative field
- Robot-assisted image guidance — da Vinci Firefly (ICG + robotic)
- AI-integrated navigation systems — automatic registration, predictive tissue identification
- Intraoperative MRI (iMRI) — real-time brain tumour margin assessment during craniotomy
ICG (Indocyanine Green) in Surgery
►
Definition
Indocyanine Green (ICG) is a fluorescent dye that binds to plasma proteins and emits near-infrared (NIR) fluorescence, used for real-time visualisation of tissue perfusion, lymphatics, and anatomy during surgery.
Mechanism
ICG is exclusively excreted in bile (no renal excretion) → concentrates in biliary tree → used for biliary mapping
Half-life: 3–5 minutes → short window but repeatable dosing
Physiological Basis of Applications
| Property | Surgical Application |
|---|---|
| Binds albumin → intravascular marker | Fluorescence angiography — perfusion assessment |
| Excreted exclusively in bile | Biliary mapping — bile duct visualisation |
| Fluorescence intensity ∝ perfusion | Anastomotic viability, flap perfusion, bowel perfusion |
| Taken up by hepatocytes then tumour tissue retains it longer | Hepatic tumour identification |
Uses in Surgery
| Field | Applications of ICG |
|---|---|
| Hepatobiliary | Bile duct visualisation, segmental liver mapping, bile leak detection, tumour margin identification |
| Gastrointestinal | Assessment of bowel perfusion and anastomotic viability in colorectal/gastric surgery |
| Vascular | Evaluation of tissue perfusion, flap viability, detection of ischaemia, bypass graft patency |
| Oncologic | Sentinel lymph node mapping (breast, gastric, colorectal cancers) |
| Transplant | Assessment of graft perfusion (liver, kidney) |
| Plastic & Reconstructive | Flap perfusion and viability assessment |
| Urology | Visualisation of ureters and renal vasculature during pelvic surgery |
Dose
- Perfusion assessment (fluorescence angiography): 0.2–0.5 mg/kg IV
- Biliary mapping (fluorescence cholangiography): 2.5–5 mg IV given 45–60 min before surgery
- Sentinel node mapping: 0.5–1 ml of 0.5 mg/ml injected peritumoural
Advantages
- Real-time, non-invasive perfusion assessment
- Reduces ischaemic complications — detects microvascular compromise not visible to naked eye
- No ionising radiation
- Short half-life allows repeat assessment
- Enhances anatomical visualisation of biliary tree without bile duct puncture
Limitations
- Requires specialised NIR camera system (not universally available)
- Limited tissue penetration (~5–10 mm) — deep structures not visualised
- Contraindicated in iodine allergy (iodine-containing dye)
- Transient visualisation window; background liver fluorescence if biliary mapping done too early
- False negatives in severe vasospasm
ICG-Assisted Surgery — Detailed Applications
►1. Fluorescence Angiography (Perfusion Assessment)
Principle: After IV ICG injection (0.2–0.5 mg/kg), NIR camera detects tissue perfusion in real time. Well-perfused areas appear bright; ischaemic regions appear dark.
Applications:
- Colorectal surgery: Assess bowel perfusion before anastomosis → reduces anastomotic leak rates
- Plastic/Reconstructive surgery: Evaluate flap viability and skin perfusion before inset
- Vascular surgery: Assess bypass graft patency or distal flow after revascularisation
- Gastro-oesophageal surgery: Assess gastric conduit perfusion in oesophagectomy
2. ICG Biliary Mapping (Fluorescence Cholangiography)
Principle: ICG is exclusively hepatically excreted in bile, highlighting the biliary tree under NIR imaging without contrast injection into the duct.
Technique: IV ICG 2.5–5 mg given 45–60 min pre-op; NIR camera visualises biliary anatomy in real time during dissection.
Applications:
- Laparoscopic cholecystectomy: Identify Calot’s triangle structures (cystic duct, CBD, CHD); detect anomalous or accessory hepatic ducts; especially valuable in difficult cases (acute cholecystitis, Mirizzi syndrome)
- Liver surgery: Map segmental bile ducts; assess bile leaks post-resection
Advantage over intraoperative cholangiogram (IOC): Real-time continuous visualisation; no duct puncture; no radiation; can be repeated.
3. Sentinel Lymph Node Mapping
Peritumoral injection of ICG → lymphatic uptake → NIR camera identifies first-echelon (sentinel) nodes glowing green → targeted biopsy without formal lymphadenectomy.
Used in: breast cancer, gastric cancer, colorectal cancer, melanoma.
4. Hepatic Tumour Identification
Hepatocytes take up ICG and excrete it; tumour cells retain ICG longer → tumour nodules appear brighter than surrounding liver tissue. Used for detecting small HCC nodules and intrahepatic metastases during liver resection.
CT Scan
►
Principle
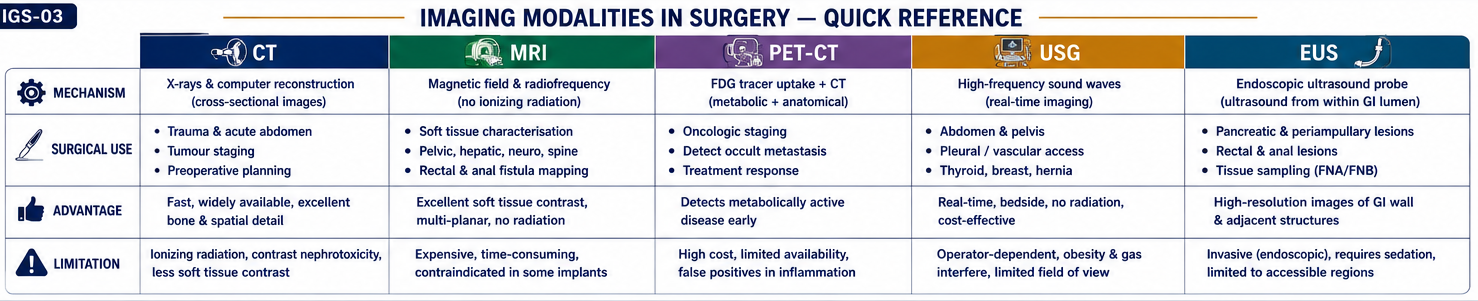
CT uses X-ray attenuation to generate cross-sectional images. The X-ray tube rotates around the patient; different tissues absorb X-rays differently (bone = white/high attenuation; soft tissue = grey; air/fat = black/low attenuation). Computer algorithms reconstruct 3D cross-sectional images from the acquired data.
Types of CT Scanners
| Type | Description |
|---|---|
| Conventional (Axial) | Single slice per rotation; older type |
| Spiral / Helical CT | Continuous rotation + table movement → helix of data → faster 3D reconstruction |
| Multidetector CT (MDCT) | Multiple detector rows → many slices per rotation → high speed and resolution; current standard |
| HRCT | Thin slices (1–2 mm) — excellent lung and bone detail |
| CT Angiography (CTA) | IV contrast → visualises vessels, stenosis, aneurysm |
| Dual-energy CT (DECT) | Two X-ray energy levels → differentiates materials (stone composition, iodine, urate) |
Surgical Uses
| System / Area | CT Use |
|---|---|
| Head | Intracranial bleed, skull fractures, tumours, hydrocephalus |
| Chest | Pulmonary embolism (CTPA), lung tumours, mediastinal mass, pneumothorax |
| Abdomen | Appendicitis, pancreatitis (CT Severity Index), trauma, abscess, bowel obstruction |
| Vascular | CT angiography for AAA, aortic dissection, mesenteric ischaemia |
| Oncology | Tumour staging, response assessment, metastasis detection |
| Guided procedures | CT-guided biopsy, abscess drainage, lesion localisation |
Advantages
- High spatial resolution — excellent anatomical detail
- Fast and widely available
- 3D reconstruction possible for surgical planning
- Detects bone, soft tissue, and vascular lesions simultaneously
Disadvantages
- Ionising radiation — especially important in children and repeated scans
- Iodine contrast risk — nephrotoxicity, allergy
- Less sensitive than MRI for soft tissue characterisation
- Not portable; patient must go to scanner
MRI (Magnetic Resonance Imaging)
►Principle
MRI uses a strong magnetic field and radiofrequency (RF) pulses to align and then perturb hydrogen proton nuclei in tissue. As protons relax back to alignment, they emit RF signals that are detected and used to construct images. Different tissues have different T1 and T2 relaxation times, providing tissue contrast without ionising radiation.
Key MRI Sequences in Surgery
| Sequence | Use |
|---|---|
| T1-weighted | Anatomy; fat = bright; post-contrast enhancement of tumours/abscesses |
| T2-weighted | Fluid = bright; excellent for oedema, ligaments, soft tissue tumours |
| STIR (Short TI Inversion Recovery) | Fat suppression — bone marrow oedema, soft tissue pathology |
| FLAIR | CSF suppressed — periventricular and cortical lesions (MS, encephalitis) |
| DWI (Diffusion-Weighted) | Detects restricted diffusion — acute stroke, abscess, malignancy |
| MRCP | Non-invasive biliary and pancreatic duct imaging (stones, strictures) |
| MR Angiography (MRA) | Vessel imaging without catheterisation |
Surgical Uses
| System | MRI Application |
|---|---|
| Brain & Spine | Tumours, demyelination, stroke, trauma, disc prolapse, cord compression |
| Abdomen / Pelvis | Liver lesions (HCC, metastases), rectal cancer staging (TME planning), pelvic tumours, fistula-in-ano |
| Biliary / Pancreas | MRCP for stones, strictures, PSC, pancreatic duct anatomy |
| Musculoskeletal | Ligament, tendon, cartilage, soft tissue sarcoma |
| Breast | Screening in BRCA carriers, implant evaluation, response to neoadjuvant chemotherapy |
CT vs MRI
| Feature | CT | MRI |
|---|---|---|
| Principle | X-ray attenuation | Magnetic resonance of protons |
| Best for | Bone, lung, acute trauma, vascular | Brain, spine, soft tissues, pelvis |
| Contrast | Iodine-based | Gadolinium-based |
| Radiation | Yes | No |
| Speed | Fast (seconds–minutes) | Slow (15–60 minutes) |
| Availability | Widespread | Less available |
| Cost | Lower | Higher |
| Metallic implants | Artefact but usually safe | Pacemakers / ferromagnetic = contraindicated |
Contraindications to MRI
Absolute: Pacemaker/defibrillator; ferromagnetic aneurysm clips; cochlear implants; metallic foreign body in eye.
Relative: Claustrophobia; first trimester pregnancy; renal failure (gadolinium → nephrogenic systemic fibrosis); inability to lie still.
PET-CT
►Definition
PET-CT is a hybrid imaging technique combining metabolic information from PET (Positron Emission Tomography) with anatomical detail from CT in a single scan, providing both functional and structural data.
Principle
PET component: Uses radioactive tracers (radiopharmaceuticals) that emit positrons (β¹ particles). Commonest tracer: FDG (Fluorodeoxyglucose) — a glucose analogue. Metabolically active cells (tumours, inflammation) take up more glucose → higher FDG uptake → bright on PET (SUV = Standardised Uptake Value).
CT component: Provides anatomical localisation of the metabolic hotspots detected by PET. Fusion of both images gives precise tumour location and extent.
Surgical Applications
| Clinical Scenario | PET-CT Role |
|---|---|
| Colorectal cancer | Detection of liver and extra-hepatic metastases; restaging after chemotherapy |
| Lymphoma | Staging, treatment response assessment (Deauville criteria), PET-guided biopsy |
| Lung cancer | Staging (mediastinal nodes, distant metastases), solitary pulmonary nodule evaluation |
| Oesophageal / Gastric cancer | Distant metastasis detection; avoids unnecessary surgery |
| Thyroid cancer | Recurrence detection (FDG-avid dedifferentiated thyroid cancer) |
| Melanoma | Staging and recurrence |
| Unknown primary | Localises primary tumour in CUP (carcinoma of unknown primary) |
| Fever of unknown origin / Infection | Localises occult infection/inflammation |
Limitations
- Not reliable for HCC — variable FDG uptake (well-differentiated HCC = low uptake)
- False positives: inflammatory conditions, recent surgery, granulomas (sarcoid, TB)
- False negatives: mucinous tumours, well-differentiated carcinoids (low metabolic activity)
- High cost; limited availability; radiation exposure
- Requires fasting ≥6 hrs; blood glucose <8 mmol/L before injection
Ultrasound (USG) in Surgery
►Principle
Ultrasound uses high-frequency sound waves (2–15 MHz for diagnostic imaging) emitted by a piezoelectric transducer. Sound waves reflect differently at tissue interfaces; returning echoes are detected and processed into real-time images. No ionising radiation.
Special Surgical Applications
| Application | Detail |
|---|---|
| FAST (Focused Assessment with Sonography in Trauma) | Detects intraperitoneal fluid (blood) in 4 windows: pericardial, hepatorenal (Morrison’s pouch), splenorenal, and pelvic |
| E-FAST (Extended FAST) | Adds bilateral chest views for pneumothorax and haemothorax detection |
| Duplex Doppler | Arterial/venous flow assessment in PAD, DVT; graft surveillance |
| Intraoperative USG (IOUS) | Gold standard for lesion detection during hepatic surgery; identifies additional lesions missed preoperatively; defines tumour-vessel relationships |
| Laparoscopic USG | Hepatic tumour mapping in MIS; intraoperative lymph node assessment |
| Endoscopic USG (EUS) | Pancreatic, biliary, oesophageal pathology (see next section) |
| CEUS (Contrast-Enhanced USG) | IV microbubble contrast → improved lesion characterisation; real-time vascular phase imaging for liver lesions |
Advantages
- No ionising radiation — safe in pregnancy and children
- Real-time, portable, bedside available
- Inexpensive and widely available
- Guides procedures (biopsy, drainage, central line insertion)
Limitations
- Operator dependent — significant learning curve
- Bowel gas and obesity hamper visualisation
- Poor for deep retroperitoneal or intracranial structures
- Limited soft tissue characterisation compared to MRI
EUS (Endoscopic Ultrasound)
►Definition
Endoscopic Ultrasound (EUS) is a minimally invasive technique combining endoscopy and high-frequency ultrasonography (5–20 MHz) to produce high-resolution images of the GI wall and adjacent organs (pancreas, bile duct, lymph nodes, vessels). It can also be used for fine-needle aspiration (EUS-FNA) and therapeutic procedures.
Principle
An ultrasound transducer is built into the tip of a flexible endoscope. The endoscope is inserted into the GI lumen (oesophagus, stomach, duodenum, or rectum) → placing the probe in close proximity to the target organ. This minimises interference from air and bone, allowing high-resolution imaging of deep structures. Linear probes allow needle passage for real-time guided biopsy or drainage.
Types of EUS Scopes
| Type | View | Main Use |
|---|---|---|
| Radial EUS | 360° cross-sectional (“CT-like”) | Diagnostic imaging; wall layer evaluation |
| Linear EUS | Longitudinal view along endoscope axis | Interventional procedures: EUS-FNA, drainage, neurolysis |
Surgical Applications
| System / Region | EUS Application |
|---|---|
| Pancreas | Staging pancreatic carcinoma (tumour size, SMA/SMV/portal vein invasion); characterisation of cystic lesions; detection of small lesions missed by CT/MRI; EUS-FNA for tissue |
| Biliary system | Choledocholithiasis (CBD stones) when MRCP unavailable; distal CBD strictures and periampullary tumours |
| Oesophagus & Stomach | T staging (depth of invasion) and N staging for oesophageal and gastric cancers; guides surgical vs palliative decision |
| Submucosal lesions | Differentiates GIST, leiomyoma, lipoma, duplication cyst |
| Mediastinum / Lung | Staging of lung cancer and lymphoma via EUS-FNA of mediastinal nodes |
| Rectal cancer | T staging (uT) for local tumours; guides neoadjuvant therapy decisions |
EUS-Guided Interventions
- EUS-FNA / FNB: Tissue sampling of pancreatic masses, lymph nodes, submucosal lesions
- EUS-guided drainage: Pseudocyst cystogastrostomy; hepaticogastrostomy in biliary obstruction when ERCP fails
- Coeliac plexus neurolysis (CPN): Alcohol injection for pancreatic cancer pain via EUS guidance
- EUS-guided fiducial placement: Gold markers for stereotactic radiotherapy planning
- EUS-guided rendezvous: Combined with ERCP for difficult biliary cannulation
Advantages over Other Modalities
- Highest resolution for peripancreatic structures and GI wall layers
- Allows simultaneous tissue sampling (FNA/FNB)
- No radiation; real-time guidance
- Superior to CT/MRI for T-staging of GI tumours and small pancreatic lesions
Limitations
- Invasive (endoscopic procedure); requires sedation
- Expertise-dependent; steep learning curve
- Limited field of view compared to CT/MRI
- Cannot assess distant metastases