General Surgery Fundamentals
Surgical physiology, critical care scoring systems, perioperative management, acid–base disorders and hospital-acquired infections — the foundation every MS and DNB candidate must know cold.
Mediators of Inflammation & Role of Cytokines
►Definition
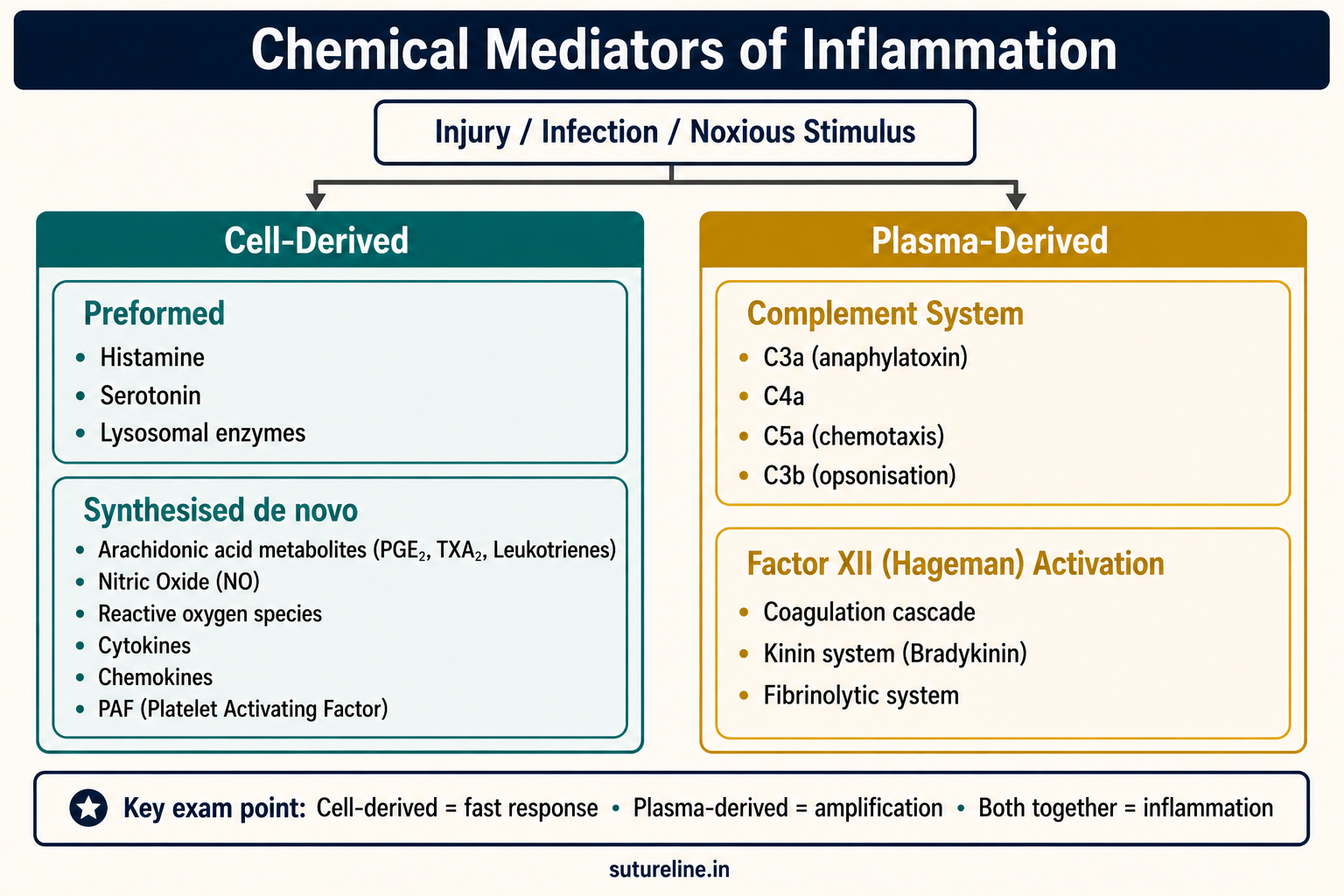
Inflammatory mediators are biologically active substances derived from host cells or plasma that initiate, amplify, regulate, and resolve the inflammatory response following injury, infection, or noxious stimuli.
Classification
A. Cell-Derived Mediators
1. Preformed (released immediately):
- Histamine — mast cells, basophils, platelets → vasodilation, ↑ permeability.
- Serotonin — platelets → vasoconstriction, platelet aggregation.
- Lysosomal enzymes — leukocyte granules → tissue destruction.
2. Synthesised de novo:
- Arachidonic acid metabolites:
- Prostaglandins (PGE₂, PGI₂) → vasodilation, pain, fever.
- Thromboxane A₂ → vasoconstriction, platelet aggregation.
- Leukotrienes (LTB₄ = chemotaxis; LTC₄, LTD₄ = bronchospasm, permeability).
- Lipoxins → resolution of inflammation.
- PAF (Platelet Activating Factor) — vasodilation, chemotaxis, ↑ permeability.
- Nitric Oxide (NO) — vasodilation, cytotoxic.
- Chemokines — leukocyte migration.
- Cytokines — IL-1, TNF-α, IL-6, IL-8 (pro-inflammatory); IL-4, IL-10, TGF-β (anti-inflammatory).
B. Plasma-Derived Mediators
- Complement system — C3a, C4a (anaphylatoxins), C5a (chemotaxis), C3b (opsonisation).
- Kinin system — Bradykinin → vasodilation, pain, ↑ permeability.
- Coagulation & fibrinolytic system — thrombin, fibrin degradation products.
Role of Cytokines in Inflammation
| Cytokine | Main Source | Key Actions |
|---|---|---|
| IL-1 | Macrophages, endothelium | Fever, ↑ adhesion molecules, acute phase proteins, proteolysis in muscle |
| TNF-α | Macrophages, T cells | Endothelial activation, fever, cachexia, shock in sepsis |
| IL-6 | Macrophages, endothelium, fibroblasts | Acute phase protein synthesis, fever, synergism with cortisol |
| IL-8 (CXCL8) | Macrophages, endothelium | Neutrophil chemotaxis and activation |
| IFN-γ | NK cells, Th1 cells | Macrophage activation, ↑ MHC expression → granuloma formation |
| IL-10 | Macrophages, T cells | Inhibits pro-inflammatory cytokines, suppresses MHC-II |
| TGF-β | Platelets, macrophages | Suppresses inflammation, promotes tissue repair & fibrosis |
| IL-4, IL-13 | Th2 cells, mast cells | Inhibit macrophage activation, promote M2 (anti-inflammatory) pathway |
Body Response to Injury
►Definition
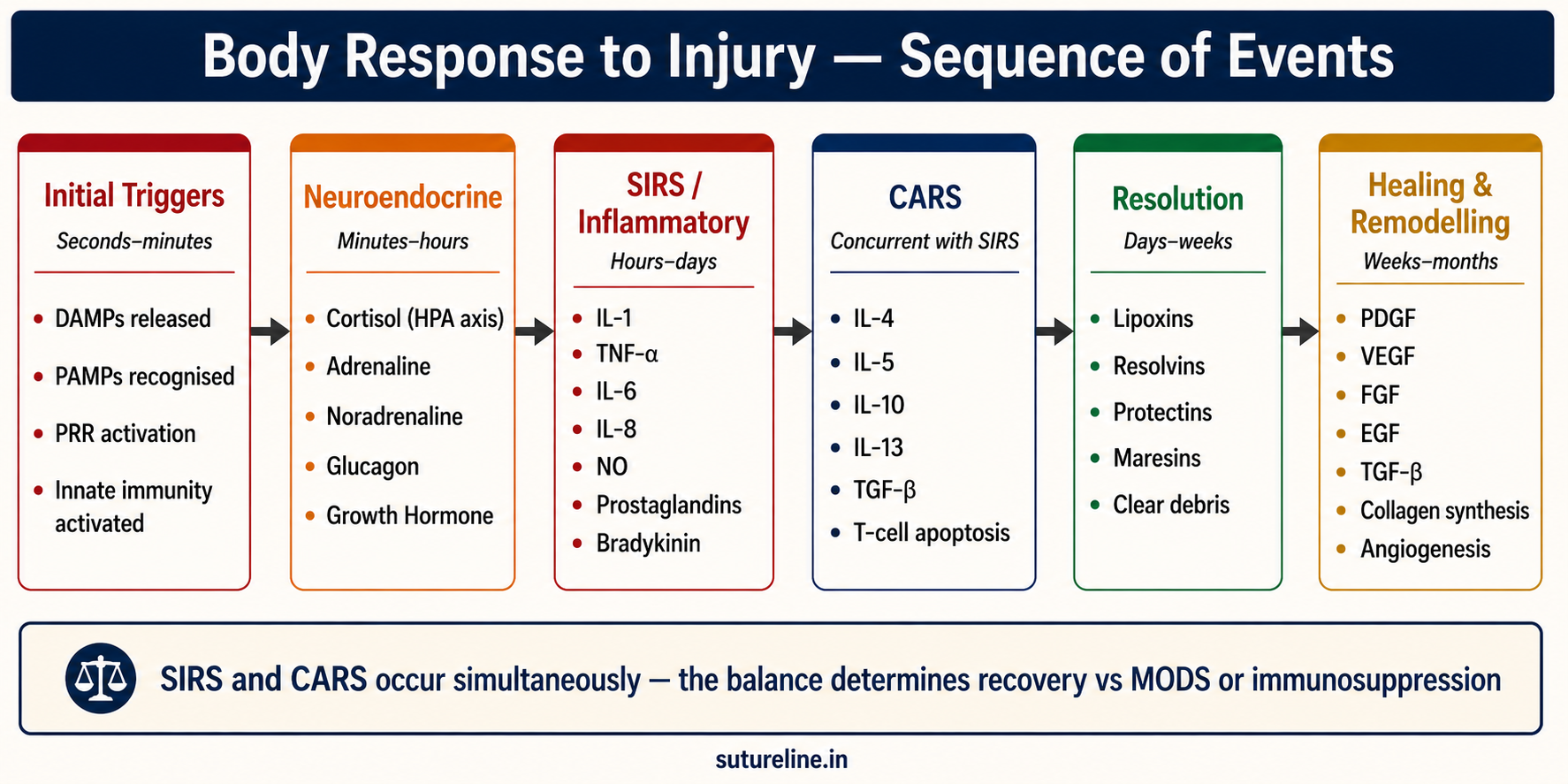
An integrated neuroendocrine, inflammatory, and metabolic reaction to tissue injury, aiming to restore homeostasis and initiate repair. SIRS and CARS occur simultaneously — the balance between them determines outcome.
Sequence of Events
| Phase | Timeframe | Main Mediators | Purpose |
|---|---|---|---|
| Initial triggers | Seconds–minutes | DAMPs | Activate immune recognition |
| Neuroendocrine | Minutes–hours | Cortisol, adrenaline, glucagon, GH | Energy mobilisation, catabolism |
| SIRS | Hours–days | IL-1, TNF-α, IL-6, IL-8, NO, PGs, bradykinin | Vasodilation, fever, leukocyte recruitment |
| CARS | Concurrent | IL-4, IL-10, IL-13, TGF-β | Suppress excess inflammation, prevent organ damage |
| Resolution | Days–weeks | Lipoxins, resolvins, protectins, maresins | Clear debris, switch to healing |
| Healing & remodelling | Weeks–months | PDGF, VEGF, FGF, EGF, TGF-β | Angiogenesis, fibroblast activation, collagen maturation |
Neuroendocrine Activation
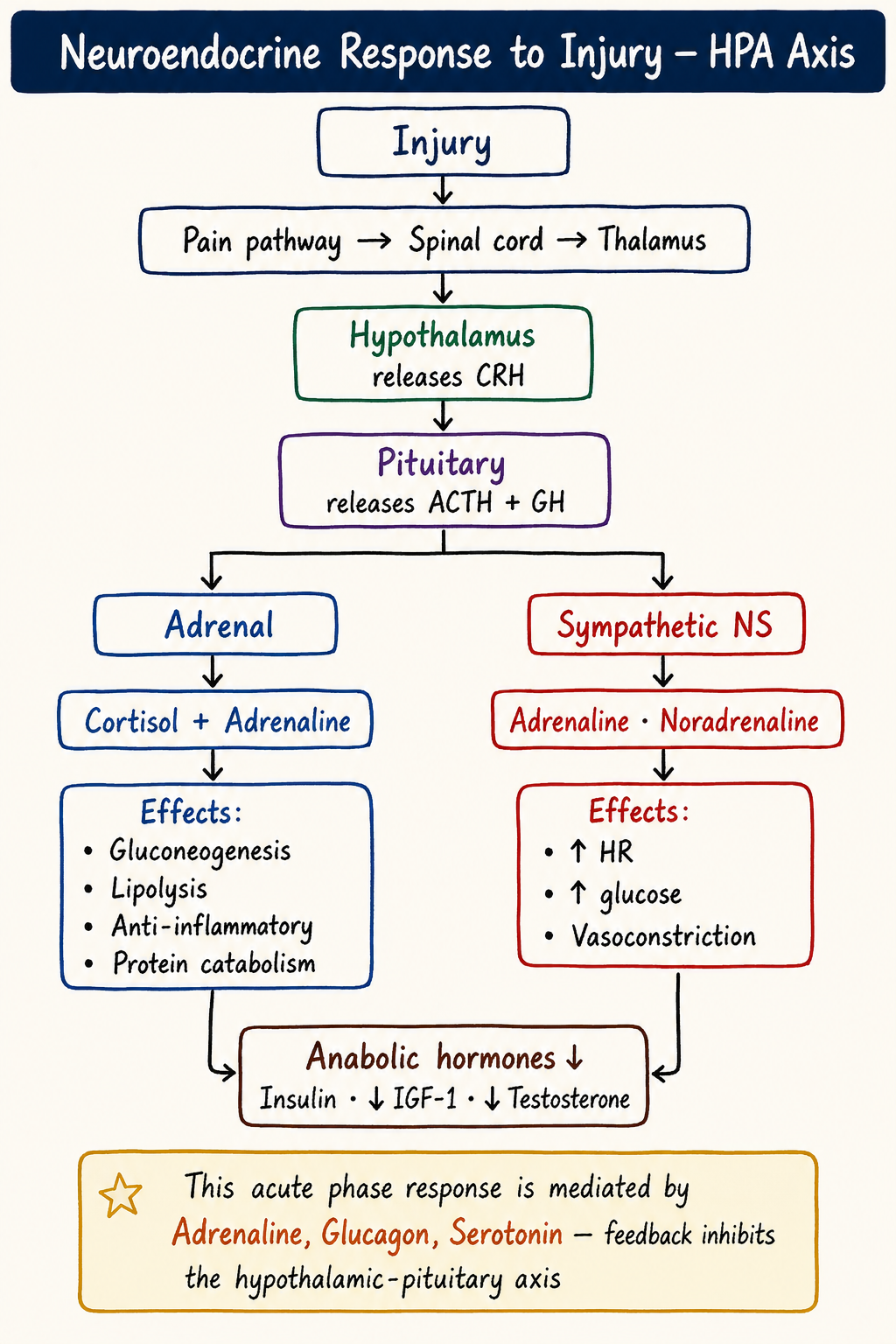
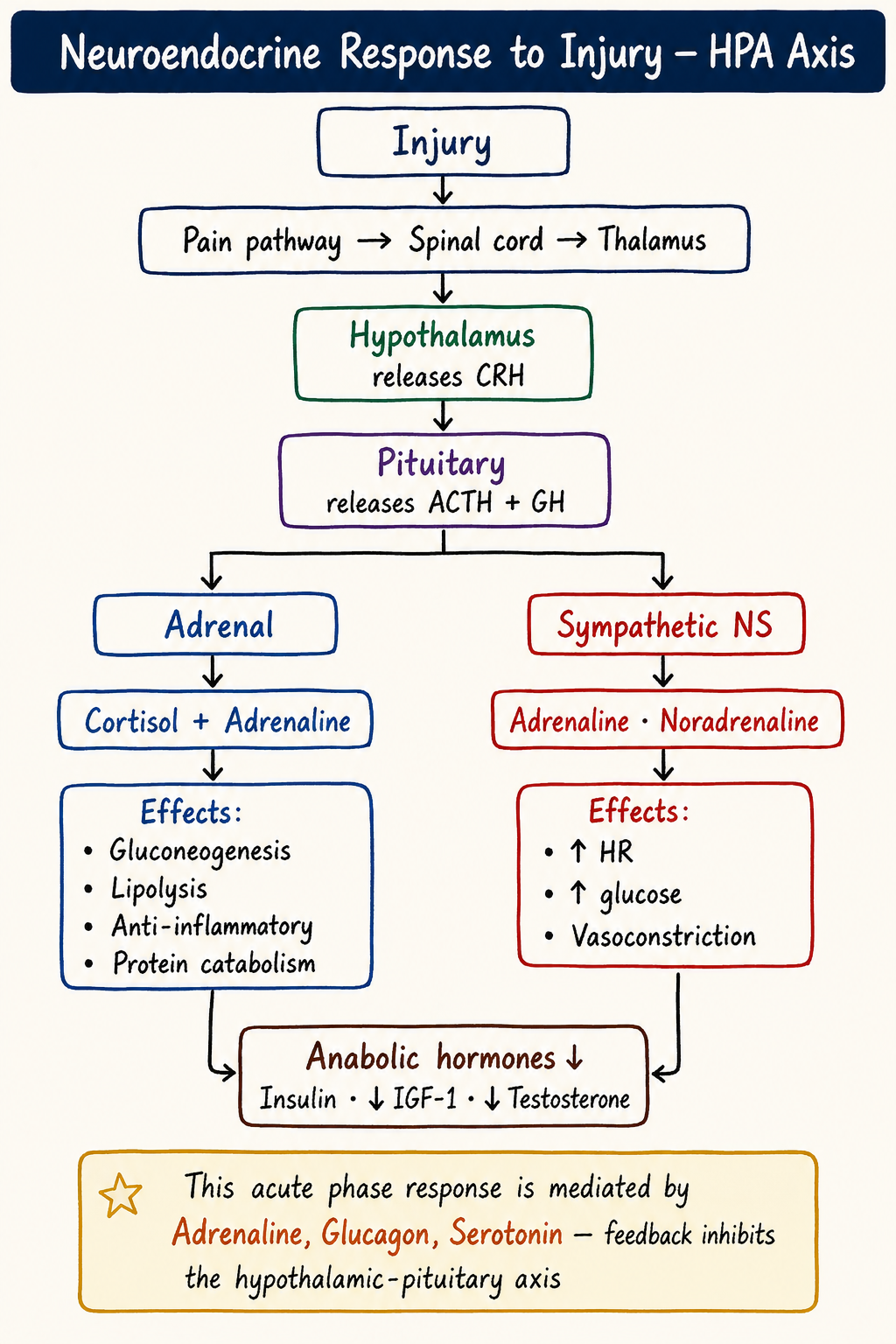
Rapid activation of the hypothalamic–pituitary–adrenal (HPA) axis and sympathetic nervous system:
- Cortisol — gluconeogenesis, protein catabolism, immune modulation.
- Adrenaline (epinephrine) — glycogenolysis, lipolysis, ↑ cardiac output.
- Glucagon — hepatic glucose release.
- Growth hormone (GH) — lipolysis, insulin antagonism, pro-inflammatory effect.
- Net metabolic effect: ↑ glucose, ↑ free fatty acids, ↑ amino acids for repair.
High-Yield Summary Table
| Phase | Key Mediators | Function |
|---|---|---|
| Neuroendocrine | Cortisol, adrenaline, glucagon, GH | Energy mobilisation, immune modulation |
| Inflammatory | IL-1, TNF-α, IL-6, IL-8, NO, prostaglandins, bradykinin | Vasodilation, permeability, leukocyte recruitment |
| Anti-inflammatory | IL-4, IL-10, IL-13, TGF-β | Suppress macrophage activity, promote repair |
| Metabolic reprioritisation | GH, cortisol | Muscle proteolysis, acute phase proteins |
| Resolution | IL-4, IL-13, resolvins, SPMs | Clear debris, restore homeostasis |
Cellular Response to Injury
►Definition
The sum of molecular, structural, metabolic, and functional changes within cells following noxious stimuli, aiming to restore homeostasis, initiate repair, or — if injury is severe — lead to cell death.
I. Classical Cellular Adaptations (Reversible)
- Hypertrophy — ↑ cell size.
- Hyperplasia — ↑ cell number.
- Atrophy — ↓ size/function.
- Metaplasia — replacement by another cell type.
II. Reversible vs Irreversible Injury
| Feature | Reversible | Irreversible |
|---|---|---|
| Morphology | Hydropic change, fatty change, membrane blebs | Nuclear pyknosis, karyolysis, karyorrhexis |
| Mitochondria | Swelling (reversible) | Flocculent densities, rupture |
| Calcium | Mild influx | Massive Ca²&spplus; influx → enzyme activation |
| Membrane | Bleb formation | Disruption → leakage of cell contents |
| Outcome | Recovery if stimulus removed | Cell death (necrosis or apoptosis) |
III. Cell Death — Necrosis vs Apoptosis
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Nature | Uncontrolled, pathological | Programmed, physiological or pathological |
| Inflammation | Yes — triggers inflammatory response | No — phagocytosis without inflammation |
| Cell membrane | Ruptured | Intact (apoptotic bodies formed) |
| Triggers | Ischaemia, toxins, trauma | Caspase activation, p53, withdrawal of growth factors |
| Surgical significance | Source of DAMPs, amplifies SIRS | Normal tissue turnover, tumour suppression |
IV. Modern Immuno-Metabolic Response
Initial Danger Signals: DAMPs (HMGB1, HSPs, ATP, uric acid) from damaged cells activate PRRs (TLRs, NLRs) → innate immunity.
Innate Immune Activation: Macrophages, neutrophils, dendritic cells, NK cells release IL-1, TNF-α, IL-6, IL-8, interferons.
Adaptive Immune Modulation: SIRS coexists with CARS. ↑ IL-10 and IL-6, ↓ HLA-DR on monocytes, T-cell apoptosis, lymphopenia, Tregs suppress APCs and CD8&spplus; cells.
Metabolic reprioritisation: Skeletal muscle breakdown via ubiquitin–proteasome pathway → amino acids for acute-phase proteins; liver ↑ fibrinogen, CRP; peripheral insulin resistance → hyperglycaemia.
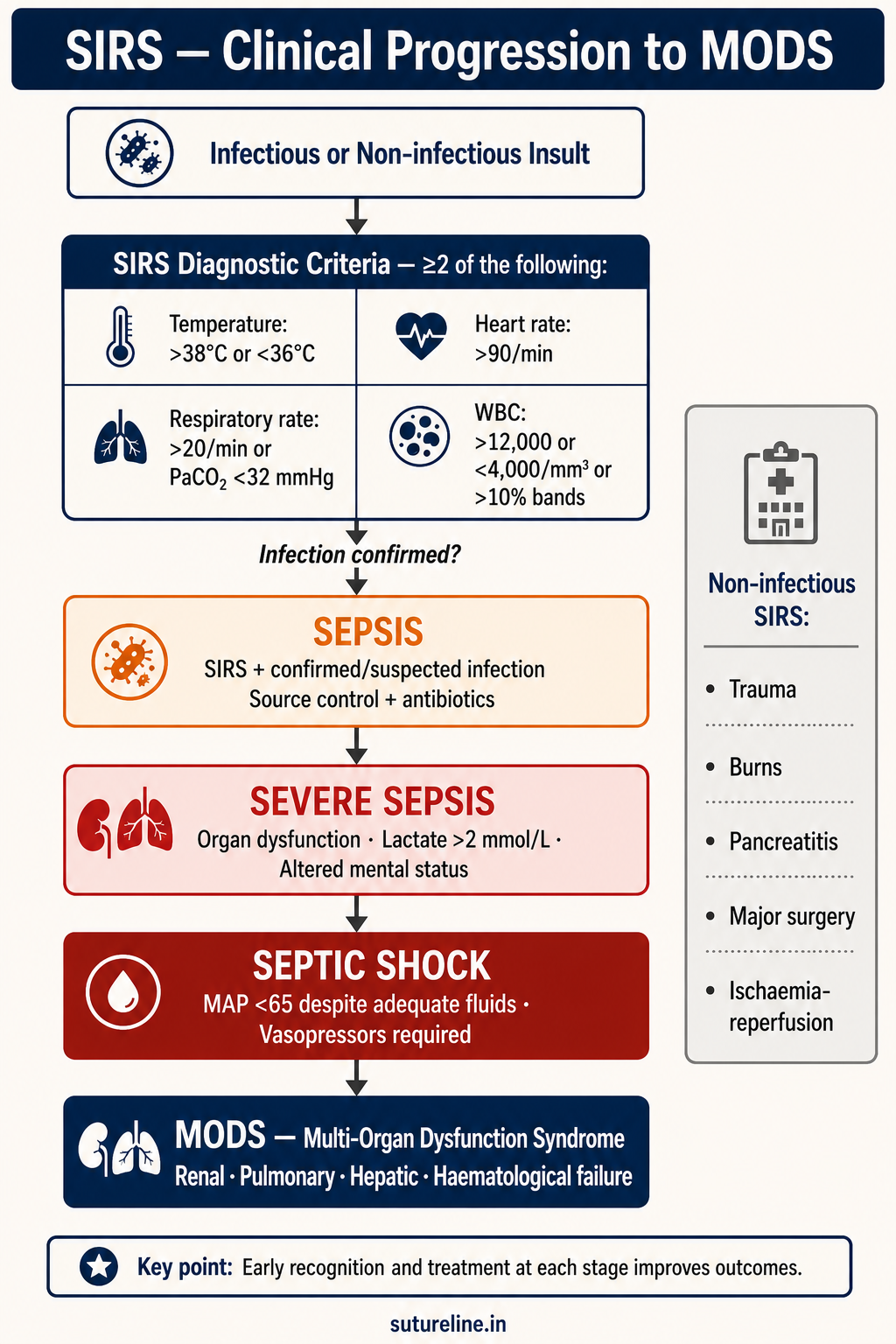
SIRS (Systemic Inflammatory Response Syndrome)
►Definition & Historical Context
A non-specific, generalised inflammatory state affecting the whole body, triggered by infectious or non-infectious insults, diagnosed when ≥2 of 4 clinical criteria are met (ACCP/SCCM Consensus, Bone et al., 1992).
Diagnostic Criteria (≥2 required)
| Parameter | Threshold |
|---|---|
| Temperature | >38.0°C or <36.0°C |
| Heart rate | >90/min |
| Respiratory rate | >20/min OR PaCO₂ <32 mmHg |
| WBC count | >12,000/mm³ OR <4,000/mm³ OR >10% bands |
Aetiology
Infectious: bacterial (esp. Gram-negative), viral, fungal, parasitic.
Non-infectious: major trauma, burns, acute pancreatitis, ischaemia–reperfusion injury, massive transfusion, severe allergic reaction, autoimmune disorders.
Pathophysiology & Mediators
- Trigger: DAMPs (tissue injury) or PAMPs (microbes) recognised by PRRs.
- Cytokine release: TNF-α, IL-1, IL-6, IL-8 → cytokine storm.
- Endothelial activation → ↑ permeability, leukocyte extravasation, microvascular thrombosis.
- Systemic effects: ↓ SVR, ↑ cardiac index (hyperdynamic phase), pulmonary oedema, neuronal injury.
- Genomic storm: 3,700 leukocyte genes altered after endotoxin; 80% of leukocyte genome altered in 28 days after severe trauma.
Relationship with CARS & Clinical Progression
- SIRS — overactivation of innate immunity.
- CARS — suppression of adaptive immunity.
- Both occur simultaneously, not sequentially.
- Excess CARS → immunoparalysis → secondary infections, poor healing, MODS.
Progression: SIRS → Sepsis (if infection) → Severe Sepsis → Septic Shock → MODS.
| Feature | SIRS | Sepsis |
|---|---|---|
| Definition | ≥2 SIRS criteria | SIRS + confirmed/suspected infection |
| Cause | Infectious or non-infectious | Infectious only |
| Prognosis | Depends on cause & control | Worse if untreated; risk of MODS |
Management
- Treat underlying cause — infection: source control + antibiotics; non-infectious: condition-specific.
- Supportive care — airway, oxygenation, ventilatory support; fluid resuscitation; vasopressors; temperature and glucose control; early enteral nutrition.
- Prevent complications — DVT prophylaxis, stress ulcer prophylaxis, early mobilisation.
DIC (Disseminated Intravascular Coagulation)
►Definition
An acquired clinicopathological syndrome characterised by widespread activation of the coagulation cascade, leading to intravascular fibrin deposition and microvascular thrombosis, with subsequent consumption of platelets and coagulation factors, resulting in a bleeding tendency. DIC is always secondary to an underlying disorder.
Pathophysiology
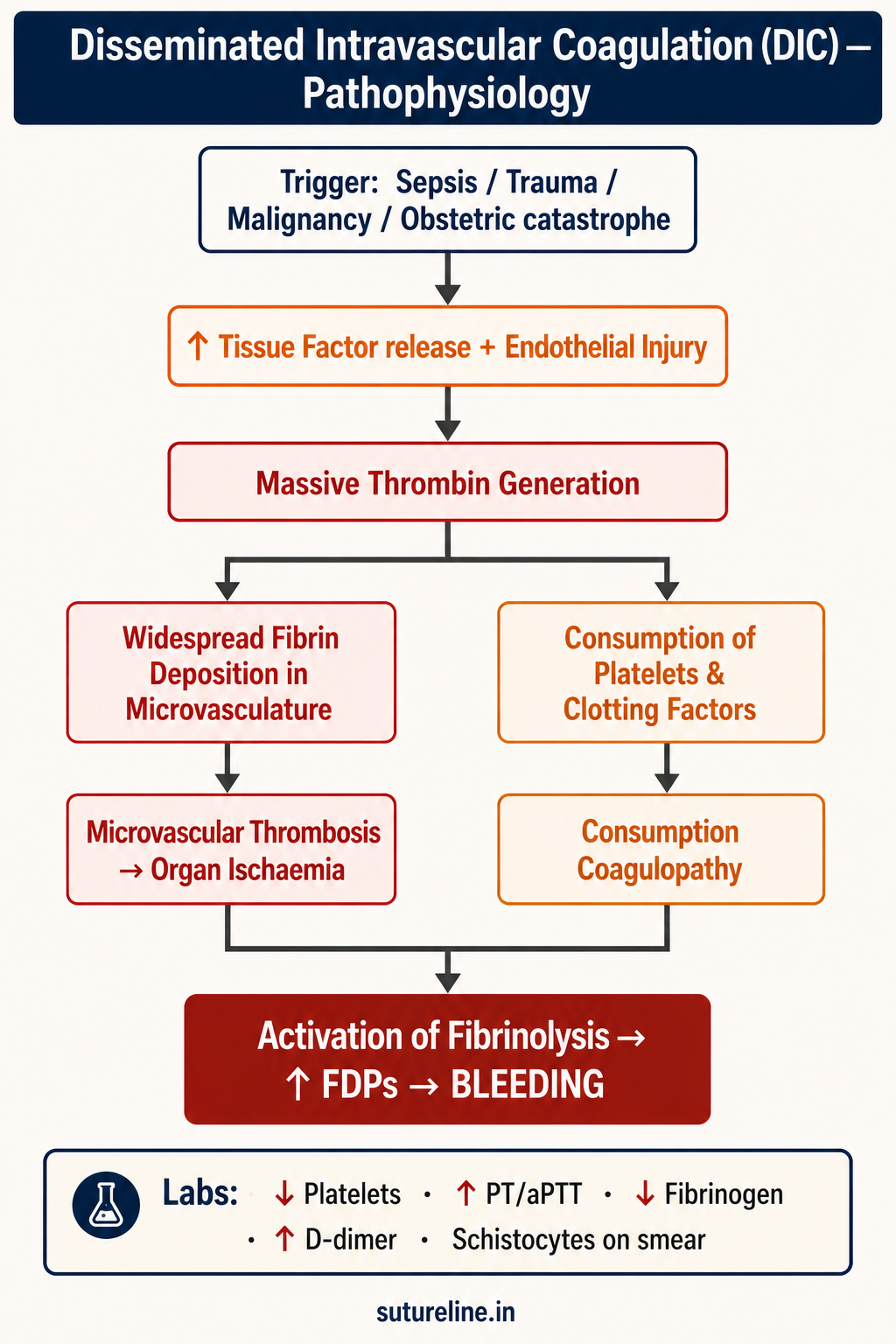
- Trigger — tissue factor release (trauma, endotoxin, tumour) → endothelial injury.
- Coagulation activation — extrinsic pathway (TF–VIIa) → massive thrombin generation → fibrin clots throughout microvasculature.
- Microvascular thrombosis — multi-organ ischaemia (MODS).
- Consumption coagulopathy — platelets and clotting factors depleted.
- Bleeding tendency — fibrinolytic system activated → ↑ FDPs → inhibit further coagulation.
Causes
- Sepsis — most common (especially Gram-negative).
- Severe trauma, burns.
- Malignancy — acute promyelocytic leukaemia, adenocarcinoma.
- Obstetric — abruptio placentae, amniotic fluid embolism, retained dead fetus.
- Massive transfusion reactions; liver failure.
Clinical Features
Thrombotic: Organ dysfunction (renal failure, respiratory distress, altered sensorium), skin necrosis, acral ischaemia.
Bleeding: Oozing from venepuncture/wound sites (classic), purpura, ecchymoses, mucosal bleeding, GI/GU haemorrhage.
Investigations
No single test is diagnostic — diagnosis is clinical + combined lab evidence.
| Parameter | Finding in DIC |
|---|---|
| Platelet count | ↓ (thrombocytopenia) |
| PT, aPTT | Prolonged |
| Fibrinogen | ↓ |
| D-dimer, FDP | ↑ (strongly suggestive) |
| Peripheral smear | Schistocytes (MAHA) |
Scoring: ISTH DIC Scoring System (≥5 = overt DIC).
Management
| Step | Key Points |
|---|---|
| 1. Treat underlying cause | Sepsis → antibiotics + source control; Obstetric → delivery; Trauma → surgical haemostasis |
| 2. Supportive measures | Haemodynamic stability; oxygenation; organ support |
| 3. Control bleeding | Platelets if <50,000/mm³ with bleeding; FFP to replenish clotting factors; Cryoprecipitate if fibrinogen <100 mg/dL; Packed RBCs for anaemia |
| 4. Control thrombosis | Low-dose heparin in predominantly thrombotic DIC (chronic DIC in malignancy) |
| 5. Adjunctive | Antithrombin III concentrates; recombinant thrombomodulin (experimental) |
ARDS (Acute Respiratory Distress Syndrome)
►Definition
A severe form of acute lung injury characterised by non-cardiogenic pulmonary oedema and refractory hypoxaemia, resulting from diffuse alveolar damage.
Etiology
Direct lung injury: Aspiration, pneumonia, lung trauma, inhalational injury, near-drowning.
Indirect (systemic): Sepsis (most common), trauma, pancreatitis, burns, massive transfusion, fat embolism.
Pathophysiology
- Inflammation at alveoli → alveolar-capillary membrane damage.
- ↑ Permeability → protein-rich alveolar oedema.
- ↓ Surfactant activity → alveolar collapse (atelectasis).
- ↓ Lung compliance, ↓ gas exchange → hypoxaemia.
- Three phases: Exudative (0–7 days) → Proliferative (7–21 days) → Fibrotic (>21 days).
Berlin Definition & Severity Classification
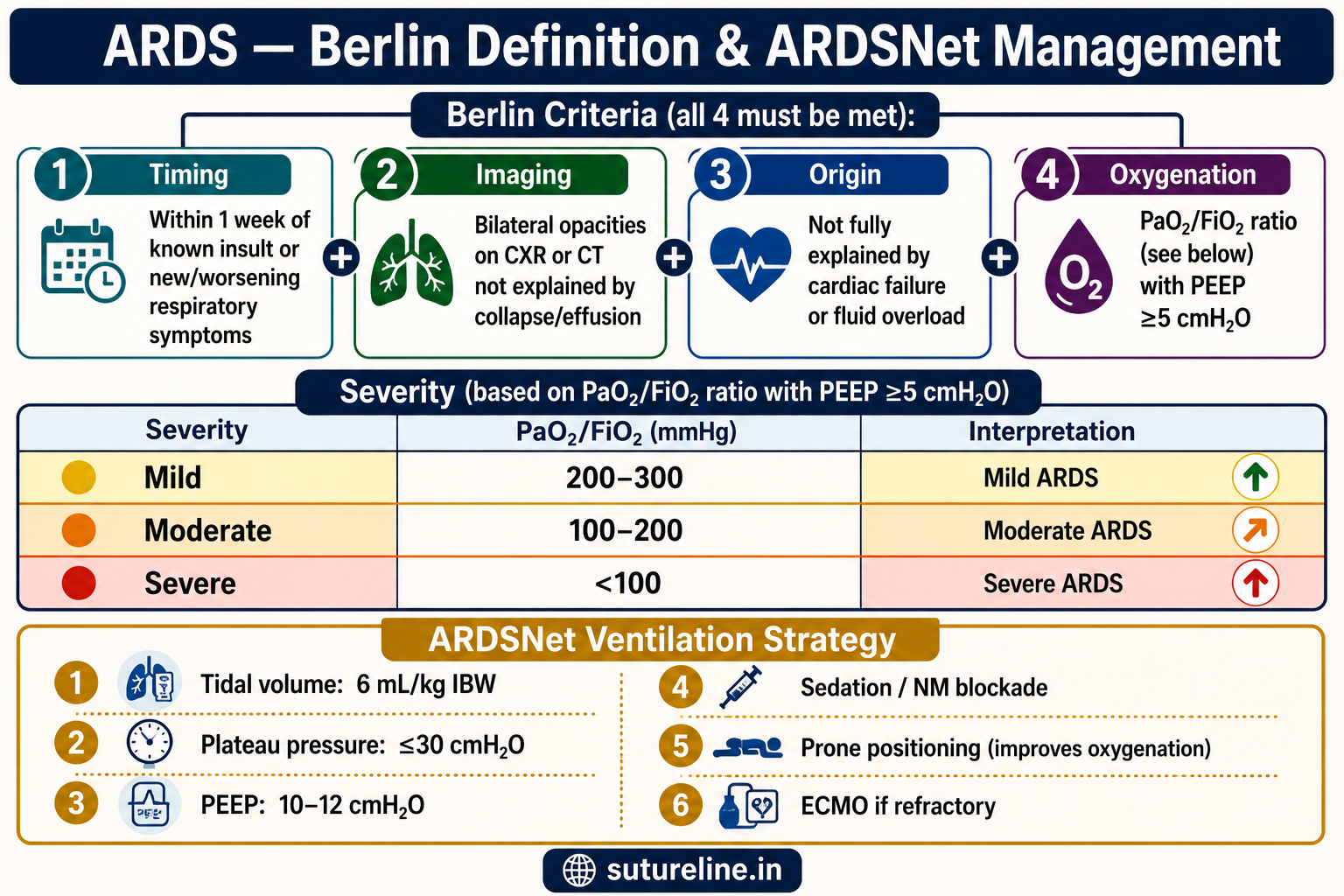
Berlin Criteria (all 4 must be present):
- Timing — within 1 week of known insult or new/worsening respiratory symptoms.
- Imaging — bilateral opacities on CXR or CT not fully explained by effusions, collapse, or nodules.
- Origin — respiratory failure not fully explained by cardiac failure or fluid overload.
- Oxygenation — PaO₂/FiO₂ ratio with PEEP ≥5 cmH₂O.
| Severity | PaO₂/FiO₂ (mmHg) | PEEP |
|---|---|---|
| Mild | 200–300 | ≥5 cmH₂O |
| Moderate | 100–200 | ≥5 cmH₂O |
| Severe | <100 | ≥5 cmH₂O |
Management
ARDSNet Ventilation Strategy:
- Low tidal volume: 6 mL/kg IBW.
- Plateau pressure: ≤30 cmH₂O.
- PEEP: 10–12 cmH₂O (adjust as needed).
- Sedation / neuromuscular blockade to improve compliance.
- Prone positioning — improves oxygenation in severe ARDS.
- If refractory: consider ECMO.
Supportive care: Treat underlying cause; conservative fluid management; nutritional support; avoid high FiO₂ and barotrauma.
Prognosis: Mortality 30–40%; better with early detection and lung-protective ventilation.
APACHE II Scoring System
►Definition
Acute Physiology and Chronic Health Evaluation II — introduced in 1985 to quantify disease severity in ICU patients and predict hospital mortality. Uses acute physiological variables, age, and chronic health status. Widely used for ICU audit, research, and outcome prediction.
APACHE II Score = Acute Physiology Score (APS) + Age Points + Chronic Health Points
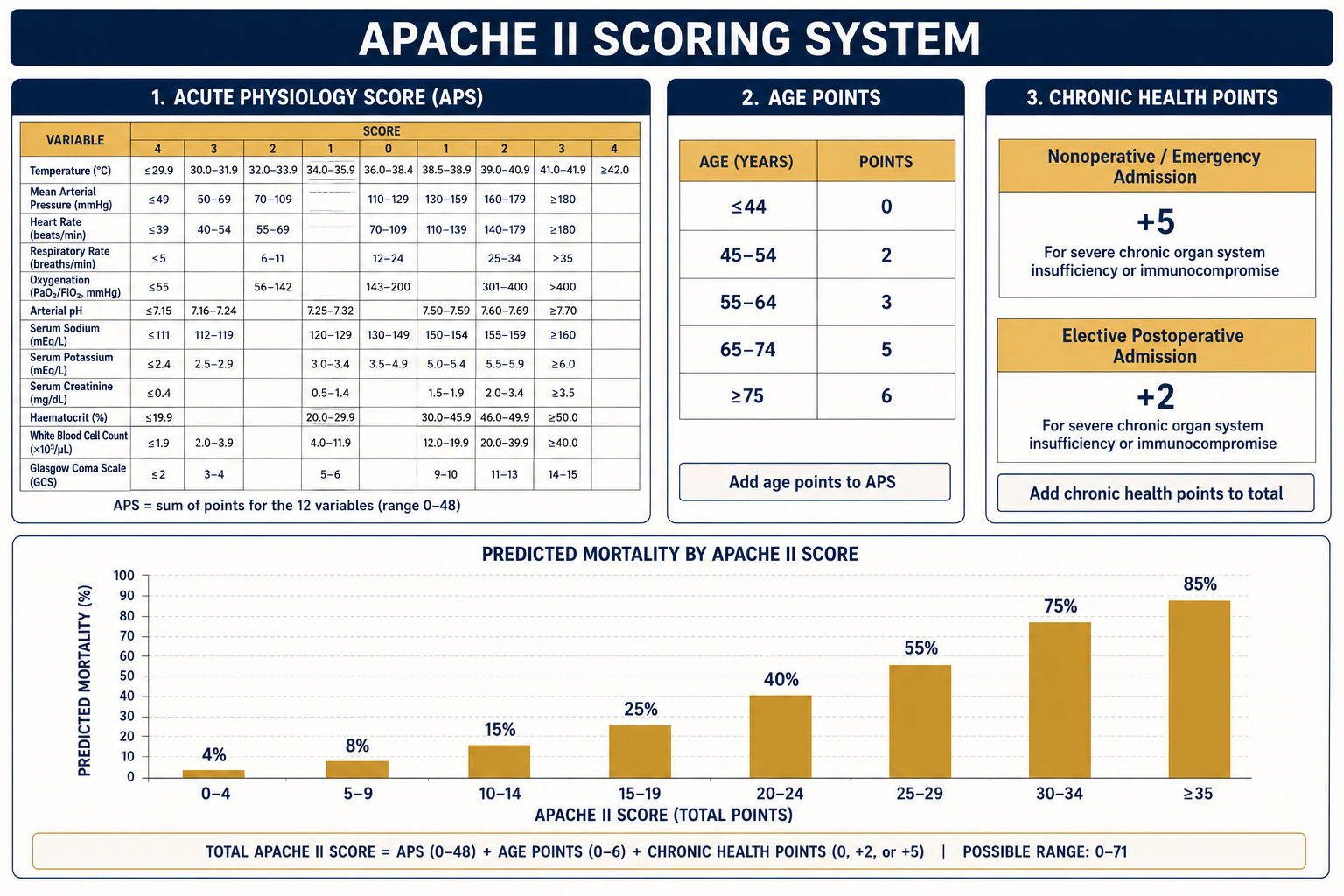
1. Acute Physiology Score (APS) — worst values in first 24 h
| Variable | Normal (Score = 0) | Score 4 (Worst) |
|---|---|---|
| Temperature (rectal °C) | 36–38.4 | <29.9 or >41 |
| Mean arterial pressure (mmHg) | 70–109 | <49 or >159 |
| Heart rate (/min) | 70–109 | <39 or >179 |
| Respiratory rate (/min) | 12–24 | <5 or >49 |
| Oxygenation | PaO₂ >70 (room air); A-a <200 (FiO₂ ≥0.5) | PaO₂ <55 or A-a >500 |
| Arterial pH / HCO₃ | 7.33–7.49 | <7.15 or >7.7 |
| Serum Na&spplus; (mmol/L) | 130–149 | <111 or >180 |
| Serum K&spplus; (mmol/L) | 3.5–5.4 | <2.5 or >7 |
| Serum creatinine (mg/dL) | 0.6–1.4 | >3.5 (double if acute RF) |
| Haematocrit (%) | 30–45 | <20 or >60 |
| WBC (×10³/µL) | 3–14.9 | <1 or >40 |
| GCS | 15 = 0 points | Score = 15 − actual GCS |
2. Age Points & 3. Chronic Health
| Age (years) | Points |
|---|---|
| ≤44 | 0 |
| 45–54 | 2 |
| 55–64 | 3 |
| 65–74 | 5 |
| ≥75 | 6 |
Chronic Health: +5 pts for nonoperative/emergency postoperative patients with severe organ insufficiency or immunosuppression; +2 pts for elective postoperative.
Mortality Prediction
| APACHE II Score | Predicted Mortality |
|---|---|
| 0–4 | ~4% |
| 5–9 | ~8% |
| 10–14 | ~15% |
| 15–19 | ~25% |
| 20–24 | ~40% |
| 25–29 | ~55% |
| 30–34 | ~75% |
| ≥35 | >85% |
Limitations: Requires accurate data within 24 h; not applicable in burns or coronary care; predicts group outcomes better than individual outcomes; not for individual treatment decisions.
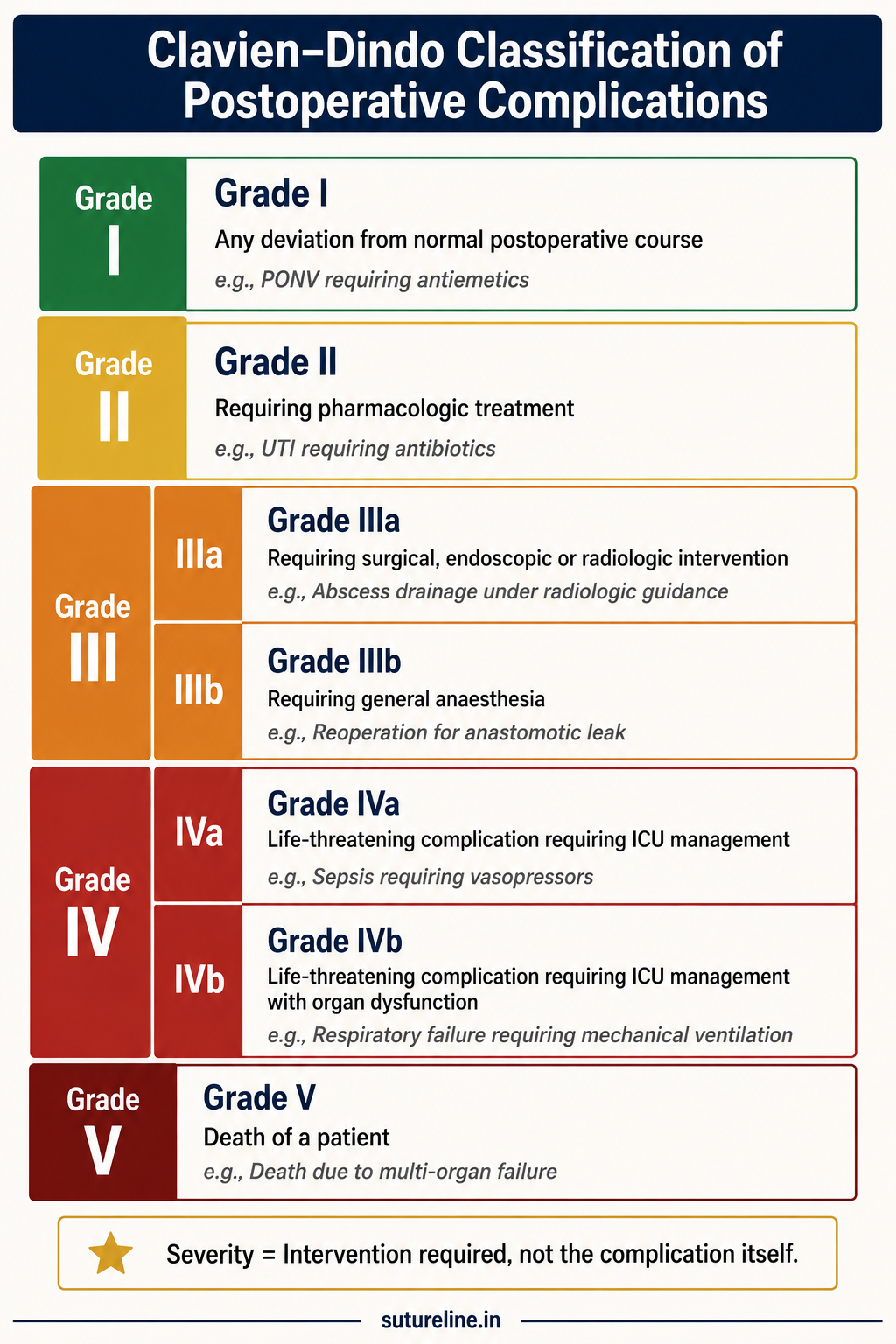
Clavien–Dindo Classification
►Definition
A standardised system to grade the severity of postoperative complications based on the type of therapy required to correct them. Proposed by Clavien et al. (1992), revised by Dindo et al. (2004).
Core Principle: Severity = intervention required to correct the complication, not the complication itself.
| Grade | Description | Example |
|---|---|---|
| I | Deviation from normal postoperative course; no pharmacological, surgical, endoscopic, or radiological intervention. Allowed: antiemetics, antipyretics, analgesics, diuretics, electrolytes, physiotherapy. | Wound infection treated by bedside dressing; fever controlled by paracetamol |
| II | Requires pharmacological treatment beyond Grade I (antibiotics, TPN, blood transfusions). | UTI needing antibiotics; postoperative anaemia requiring transfusion |
| IIIa | Surgical, endoscopic, or radiological intervention — not under general anaesthesia. | Drainage of abscess under LA |
| IIIb | Surgical, endoscopic, or radiological intervention — under general anaesthesia. | Reoperation for bleeding or anastomotic leak |
| IVa | Life-threatening complication — single-organ dysfunction requiring ICU. | Dialysis for acute renal failure; ARDS |
| IVb | Life-threatening complication — multi-organ dysfunction requiring ICU. | MODS on ventilator and inotropes |
| V | Death of the patient. | Postoperative mortality |
Suffix “d” added if patient remains disabled at discharge (e.g. stroke → Grade IVa-d). Highest grade per patient = overall morbidity score.
Performance Scores — ECOG / Karnofsky
►Definition
Performance status scales quantify a patient's functional capacity. They correlate with survival and tolerance to therapy, and guide perioperative risk assessment and eligibility for systemic treatment.
ECOG Performance Status Scale
| Grade | Description |
|---|---|
| 0 | Fully active; able to carry out all pre-disease activities without restriction. |
| 1 | Restricted in physically strenuous activity but ambulatory; able to do light/sedentary work. |
| 2 | Ambulatory and capable of self-care but unable to carry out work activities; up >50% of waking hours. |
| 3 | Capable of only limited self-care; confined to bed/chair >50% of waking hours. |
| 4 | Completely disabled; cannot carry on any self-care; totally confined to bed/chair. |
| 5 | Dead. |
Karnofsky Performance Status (Selected Values)
| Score | Description |
|---|---|
| 100 | Normal; no complaints; no evidence of disease. |
| 80 | Normal activity with effort; some symptoms. |
| 70 | Cares for self; unable to carry on normal activity/work. |
| 60 | Requires occasional assistance but can care for most needs. |
| 50 | Requires considerable assistance and frequent medical care. |
| 40 | Disabled; requires special care and assistance. |
| 30 | Severely disabled; hospitalisation indicated. |
| 10 | Moribund; fatal processes progressing rapidly. |
| 0 | Dead. |
| Feature | ECOG | Karnofsky |
|---|---|---|
| Range | 0–5 | 0–100 (10-point increments) |
| Simplicity | Simple; practical for routine use | More detailed gradations |
| Common use | Oncology trials; treatment eligibility | Palliative care; prognostication |
Surviving Sepsis Campaign
►Definitions (Sepsis-3, 2016)
- Sepsis — suspected/confirmed infection + acute organ dysfunction (↑ SOFA score ≥2).
- Septic Shock — sepsis + persistent hypotension requiring vasopressors to maintain MAP ≥65 mmHg + serum lactate >2 mmol/L after adequate fluid resuscitation.
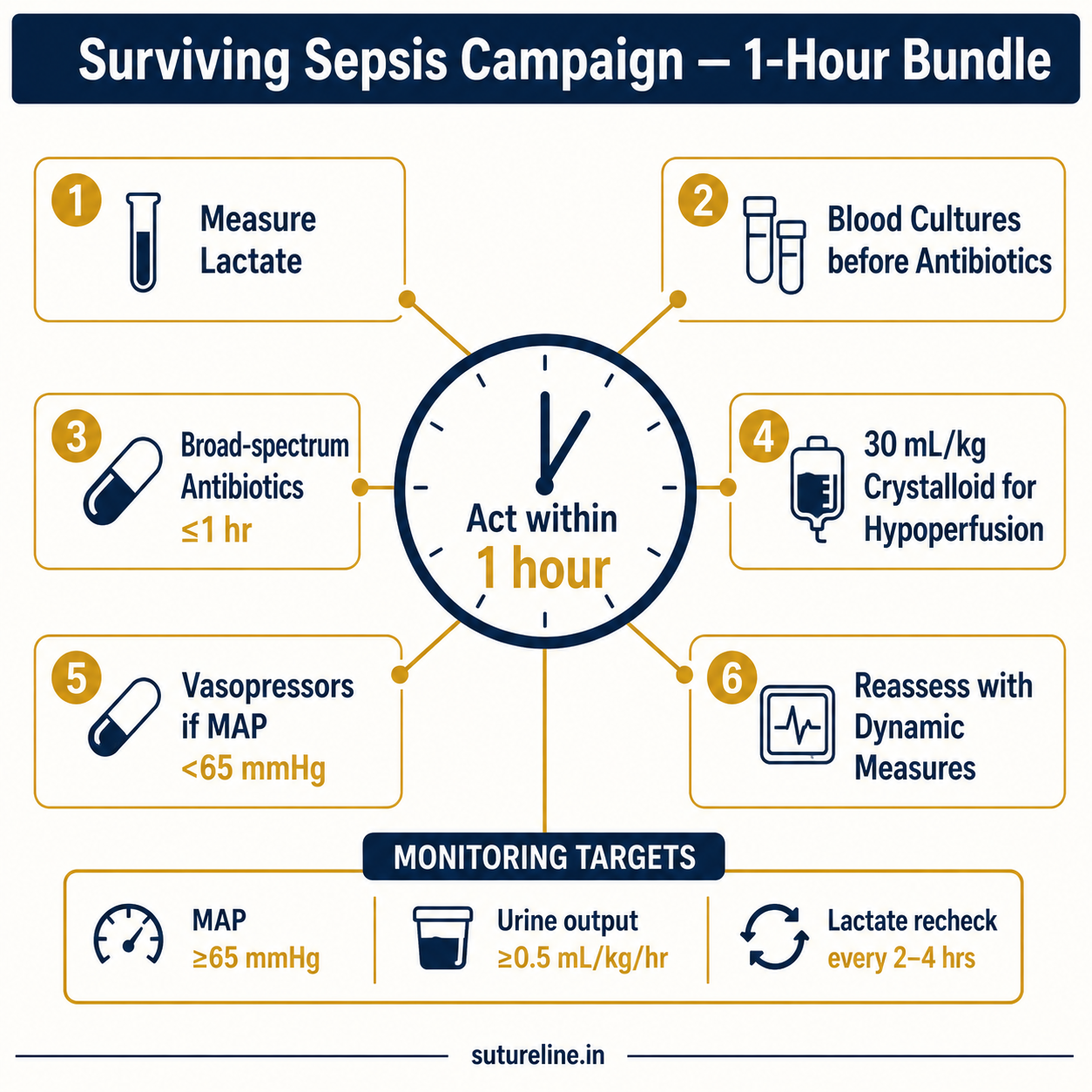
First-Hour Bundle
- Recognise sepsis (qSOFA/SOFA where appropriate).
- Measure lactate immediately; repeat if elevated.
- Obtain blood cultures before antibiotics — if this does not delay therapy.
- Broad-spectrum antibiotics ≤1 hour for septic shock or high likelihood.
- ~30 mL/kg IV crystalloids for sepsis-induced hypoperfusion within 3 h; reassess with dynamic measures.
- Vasopressors if hypotension persists → norepinephrine first-line, target MAP ≥65 mmHg.
- Source control as soon as feasible.
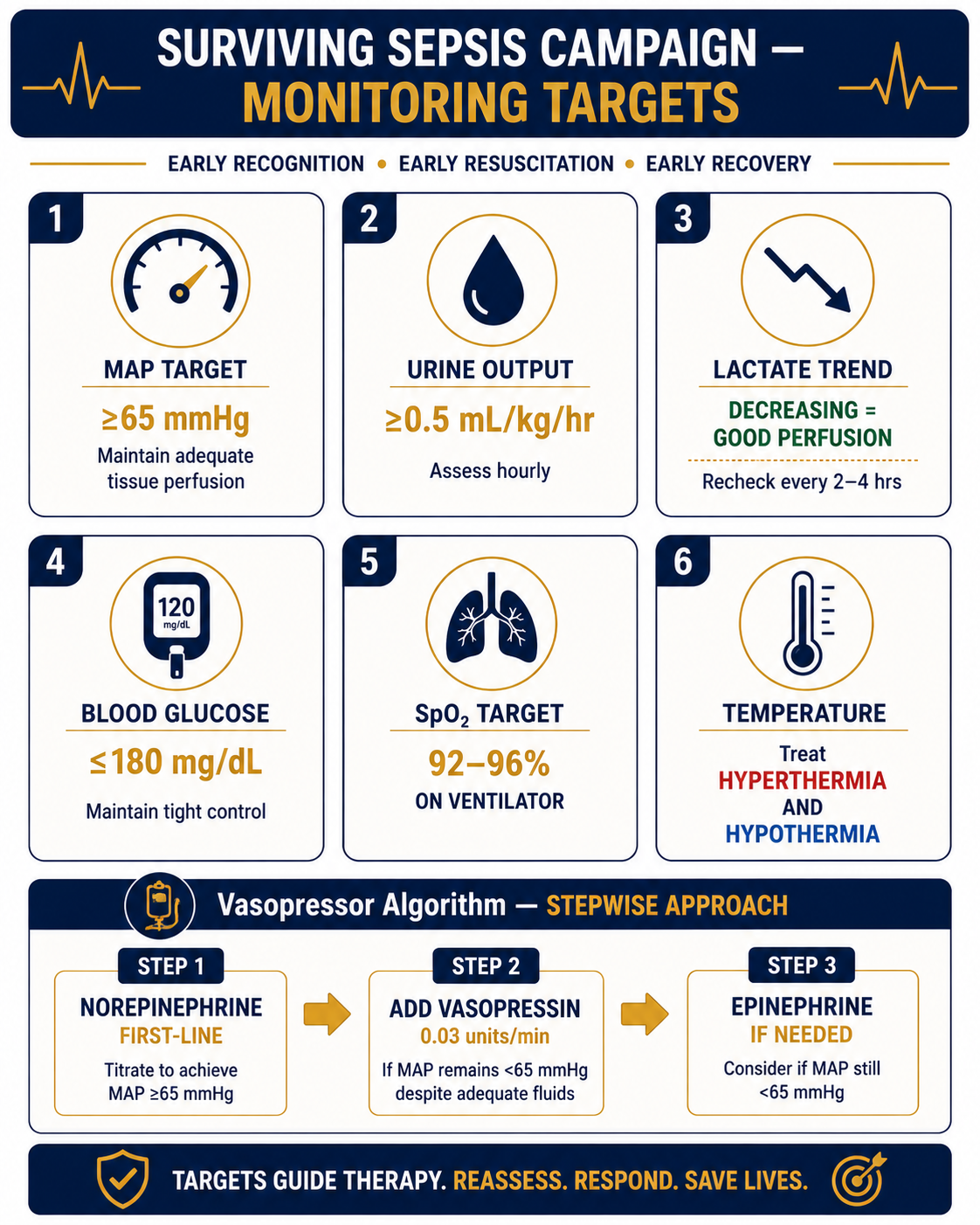
Key Targeted Recommendations
| Domain | Recommendation |
|---|---|
| Antibiotics | ≤1 hr for septic shock; avoid unnecessary antibiotics if alternate diagnosis clear |
| Fluids | Balanced crystalloids preferred over 0.9% NS; dynamic measures over static CVP |
| Vasopressors | Norepinephrine first; add vasopressin rather than escalating NE; epinephrine next |
| Lactate | Recheck every 2–4 hrs; decreasing lactate = improved perfusion |
| Corticosteroids | IV hydrocortisone only if vasopressor-dependent despite adequate fluids |
| Transfusion | Hb <7 g/dL (unless active ischaemia) |
| Targets | MAP ≥65 mmHg; urine output ≥0.5 mL/kg/hr |
WHO Surgical Safety Checklist
►Definition
A structured tool introduced by WHO (2008) as part of the Safe Surgery Saves Lives campaign. Reduces surgical morbidity and mortality by ensuring adherence to essential perioperative safety practices.
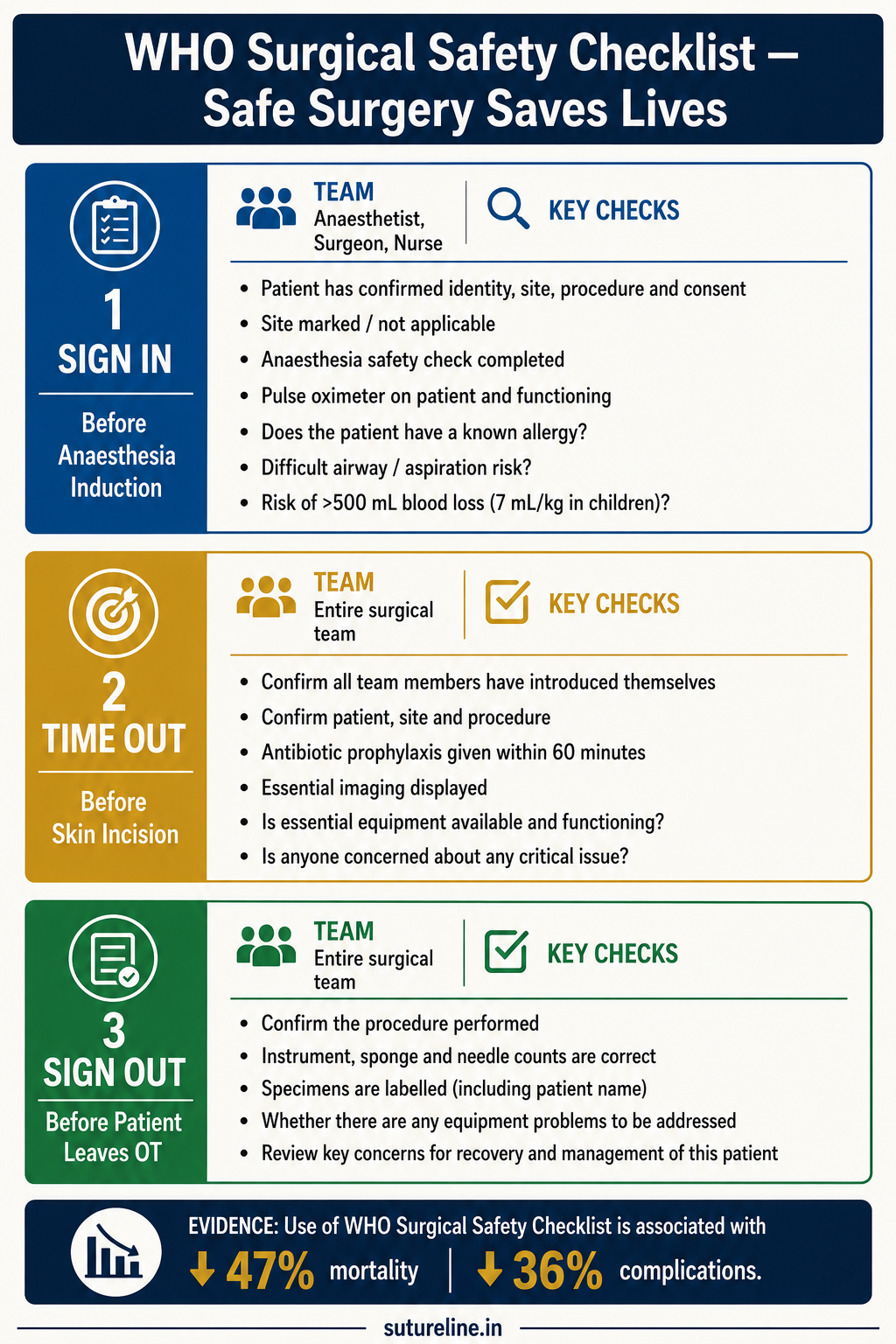
| Phase | When | Team | Key Checks |
|---|---|---|---|
| Sign In | Before anaesthesia induction | Anaesthetist, Surgeon, Nurse | Patient identity, procedure, site, consent; anaesthesia machine; allergy; airway risk; blood loss risk and product availability |
| Time Out | Before skin incision | Entire surgical team | Team introductions; reconfirm patient/procedure/site; antibiotic prophylaxis within 60 min; anticipate critical events; imaging available |
| Sign Out | Before patient leaves OT | Surgeon, Anaesthetist, Nurse | Confirm procedure; instrument/sponge/needle counts; specimen labelling; equipment problems; postoperative concerns |
Evidence of Impact
- Reduces perioperative mortality by up to 47%.
- Decreases complication rates by 36%.
- Improves team communication, cohesion, and accountability.
Postoperative Fever
►Definition
Temperature >38.5°C on ≥2 occasions at least 4 hours apart after surgery. Temporal pattern of onset is the key to diagnosis.
Differential Diagnosis — The “5 Ws”
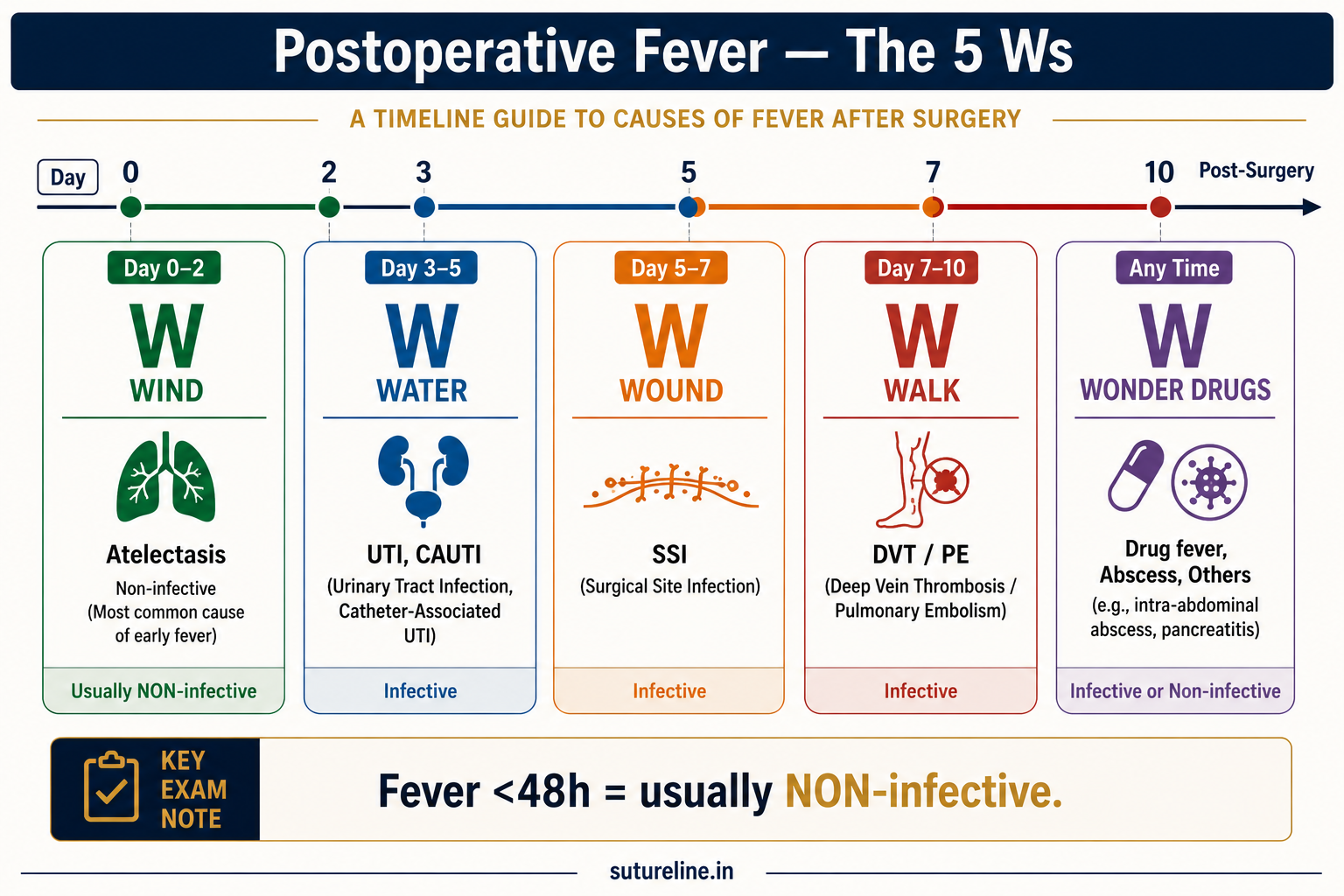
| Timing | Cause | W |
|---|---|---|
| Within 48 h (non-infective) | Atelectasis (most common), inflammatory response, transfusion reaction, malignant hyperthermia | Wind |
| Day 3–5 | UTI (catheter-associated) | Water |
| Day 5–7 | Wound infection (cellulitis 3–4 days; suppuration 7–10 days) | Wound |
| Day 7–10 | DVT / Pulmonary embolism | Walk |
| Any time | Drug fever, intra-abdominal abscess, anastomotic leak, line sepsis | Wonder drugs |
Management
- Atelectasis: Chest physiotherapy, incentive spirometry, early ambulation.
- UTI: Remove/replace catheter, antibiotics per culture.
- Wound infection: Drain pus, wound care, antibiotics.
- DVT/PE: Anticoagulation (LMWH), compression stockings.
- Drug fever: Withdraw offending agent.
Post-operative Ileus
►Definition
Temporary impairment of bowel motility after abdominal or other major surgery, in the absence of mechanical obstruction.
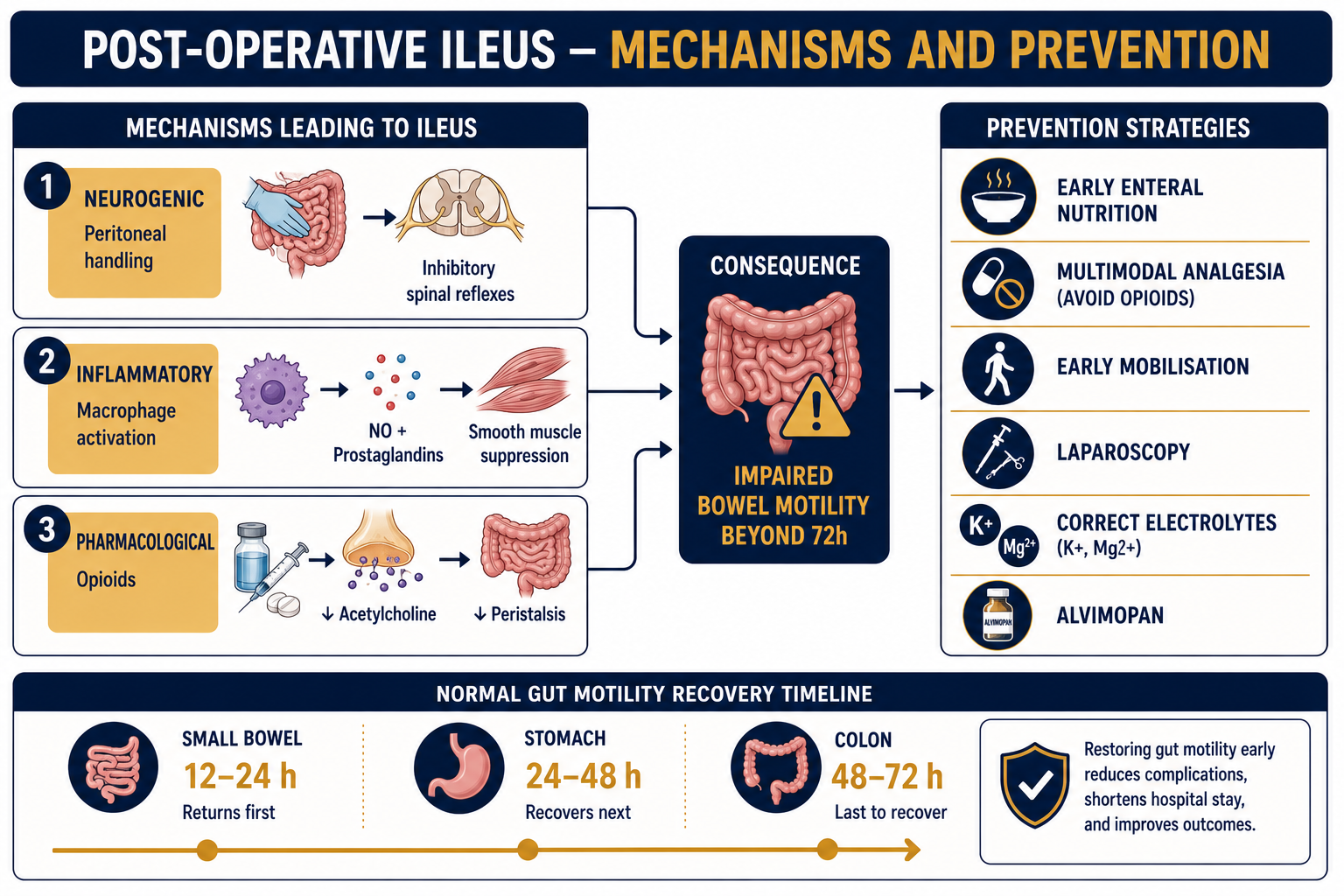
Normal Gut Motility Recovery
| Segment | Recovery |
|---|---|
| Small intestine | 12–24 h |
| Stomach | 24–48 h |
| Colon | 48–72 h |
Pathophysiology
- Neurogenic inhibition: Peritoneal handling → activation of inhibitory spinal reflexes.
- Inflammatory: Macrophage activation in intestinal muscularis releases NO, prostaglandins, cytokines → smooth muscle suppression.
- Pharmacological: Opioids activate µ-opioid receptors in enteric nervous system → ↓ acetylcholine → ↓ peristalsis.
Prevention & Management
- Early enteral nutrition within 24 h.
- Multimodal opioid-sparing analgesia (NSAIDs, paracetamol, epidural, TAP blocks).
- Early mobilisation (POD 0–1).
- Minimally invasive surgery preferred.
- Avoid routine NG tubes and drains.
- Correct electrolytes (K&spplus;, Mg²&spplus;).
- Alvimopan — peripherally acting µ-opioid receptor antagonist; licensed for post-colectomy ileus.
ERAS in GI and Colorectal Surgery
►Definition
Enhanced Recovery After Surgery (ERAS) is a multimodal, evidence-based perioperative care pathway designed to minimise surgical stress response, accelerate recovery, and reduce hospital stay without increasing readmission rates.
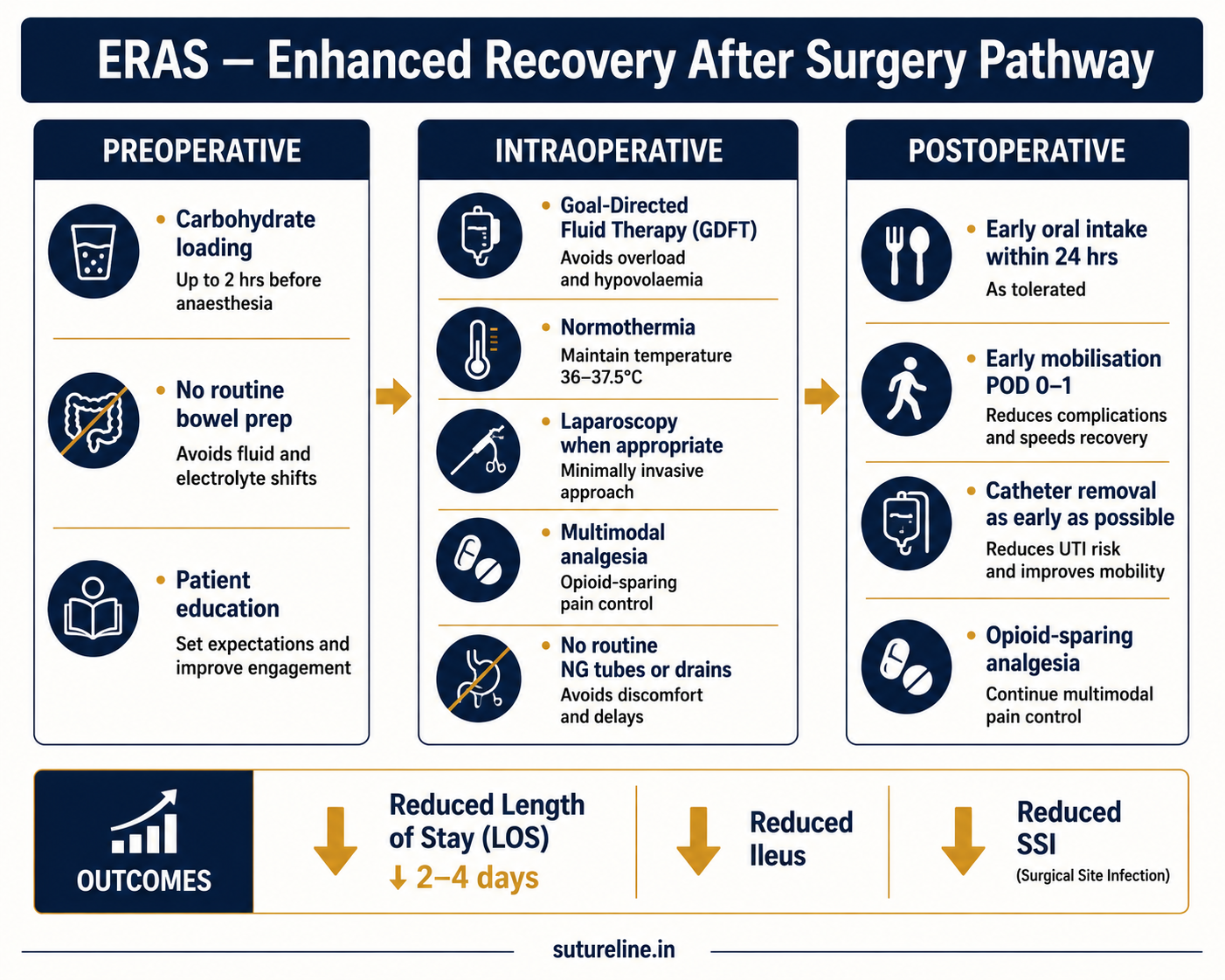
| Aspect | Conventional | ERAS |
|---|---|---|
| Fasting | Midnight NPO | Solids till 6 h; fluids till 2 h |
| Bowel prep | Routine | Selective only |
| NG tube/drains | Routine | Avoid unless indicated |
| Analgesia | Opioid-based | Multimodal, opioid-sparing |
| Mobilisation | Delayed | Early (POD 0–1) |
| Feeding | Delayed till bowel sounds | Early enteral within 24 h |
| Fluid therapy | Liberal | Goal-directed, restrictive |
Outcomes: ↓ LOS by 2–4 days; ↓ complications (ileus, infections, pulmonary); no ↑ in readmission rates; cost-effective. ERAS Society Guidelines 2022 (colorectal) — >20 evidence-based recommendations.
Ventilatory Support in Critically Ill Patients
►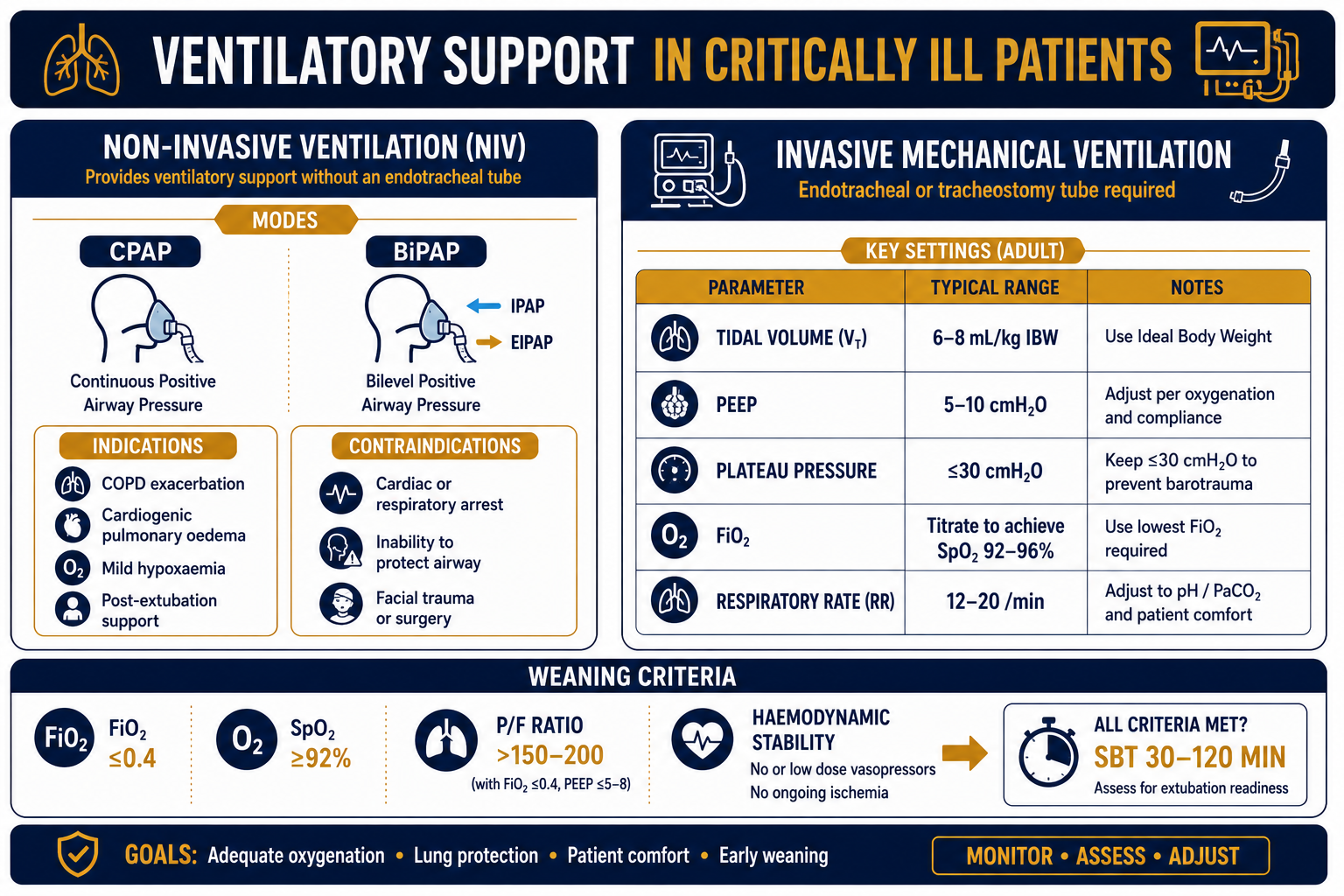
Types of Ventilatory Support
| Type | Modes | Indications | Contraindications |
|---|---|---|---|
| NIV | CPAP, BiPAP | COPD exacerbation, cardiogenic pulmonary oedema, mild hypoxaemic RF, post-extubation support | Cardiac/respiratory arrest, inability to protect airway, facial trauma, uncooperative patient |
| Invasive MV | Volume control, pressure control, SIMV, pressure support | All indications where NIV is inadequate/contraindicated; GCS <8; post-major surgery | — |
Key Ventilator Settings
| Parameter | Standard Setting | Notes |
|---|---|---|
| Tidal volume | 6–8 mL/kg IBW (6 mL/kg in ARDS) | Low tidal volume = lung protection |
| PEEP | 5–10 cmH₂O | Prevents alveolar collapse; improves FRC |
| Plateau pressure | ≤30 cmH₂O | Marker of static lung compliance |
| FiO₂ | Titrate to SpO₂ 92–96% | Avoid prolonged high FiO₂ (O₂ toxicity) |
| Respiratory rate | 12–20/min | Adjust to target PaCO₂ |
Weaning: FiO₂ ≤0.4, SpO₂ ≥92%, PF ratio >150–200, PEEP ≤5–8, haemodynamic stability, adequate spontaneous effort → Spontaneous Breathing Trial (SBT) 30–120 min → extubate if successful.
Hyperbaric Oxygen Therapy (HBOT)
►Definition
Intermittent inhalation of 100% oxygen at a pressure >1 ATA (usually 2–3 ATA) inside a pressurised chamber. Results in supraphysiological oxygen delivery by increasing dissolved O₂ in plasma (Henry's law).
Mechanisms of Action
| Mechanism | Effect |
|---|---|
| Hyperoxygenation | PaO₂ may rise >1500 mmHg; O₂ delivery to ischaemic tissues independent of Hb |
| Neovascularisation | Promotes fibroblast proliferation, collagen synthesis, angiogenesis |
| Enhanced leukocyte killing | Restores O₂-dependent phagocytosis in neutrophils |
| Oedema reduction | Hyperoxic vasoconstriction without compromising oxygenation |
| Toxin inhibition | Inhibits Clostridium; reduces α-toxin production |
| Antibiotic synergy | Synergistic with aminoglycosides, quinolones |
Surgical Indications
- Diabetic foot ulcers (refractory to standard care)
- Osteoradionecrosis (Marx protocol)
- Necrotising soft tissue infections — adjunct to debridement + antibiotics
- Compromised skin flaps and grafts
- Chronic osteomyelitis (refractory)
- Carbon monoxide poisoning; gas gangrene
Protocol: 2–3 ATA; 60–120 min/session; 20–40 sessions for chronic conditions.
OT Design & Layout
►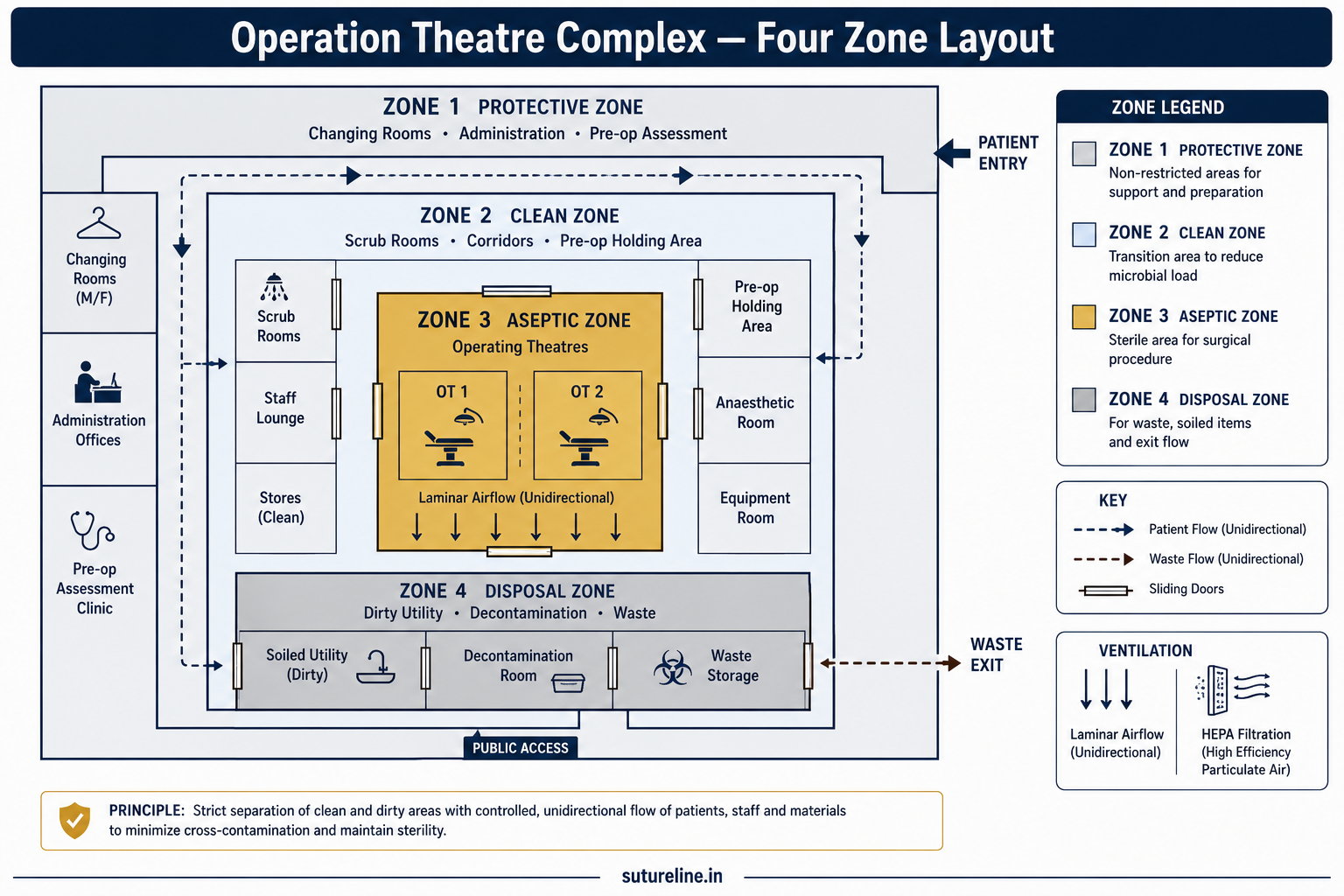
Four-Zone Layout (Least to Most Sterile)
| Zone | Description | Examples |
|---|---|---|
| 1. Protective | Entry zone; prevents outside contamination | Changing rooms, pre-op rooms, admin, sterile store |
| 2. Clean | Transition for personnel in OT attire | Scrub rooms, pre-op holding area, corridors |
| 3. Aseptic | Where operations are performed under strict asepsis | Operating theatre, instrument trolley area |
| 4. Disposal | Removal of soiled instruments, linen, waste | Dirty utility room, waste disposal area |
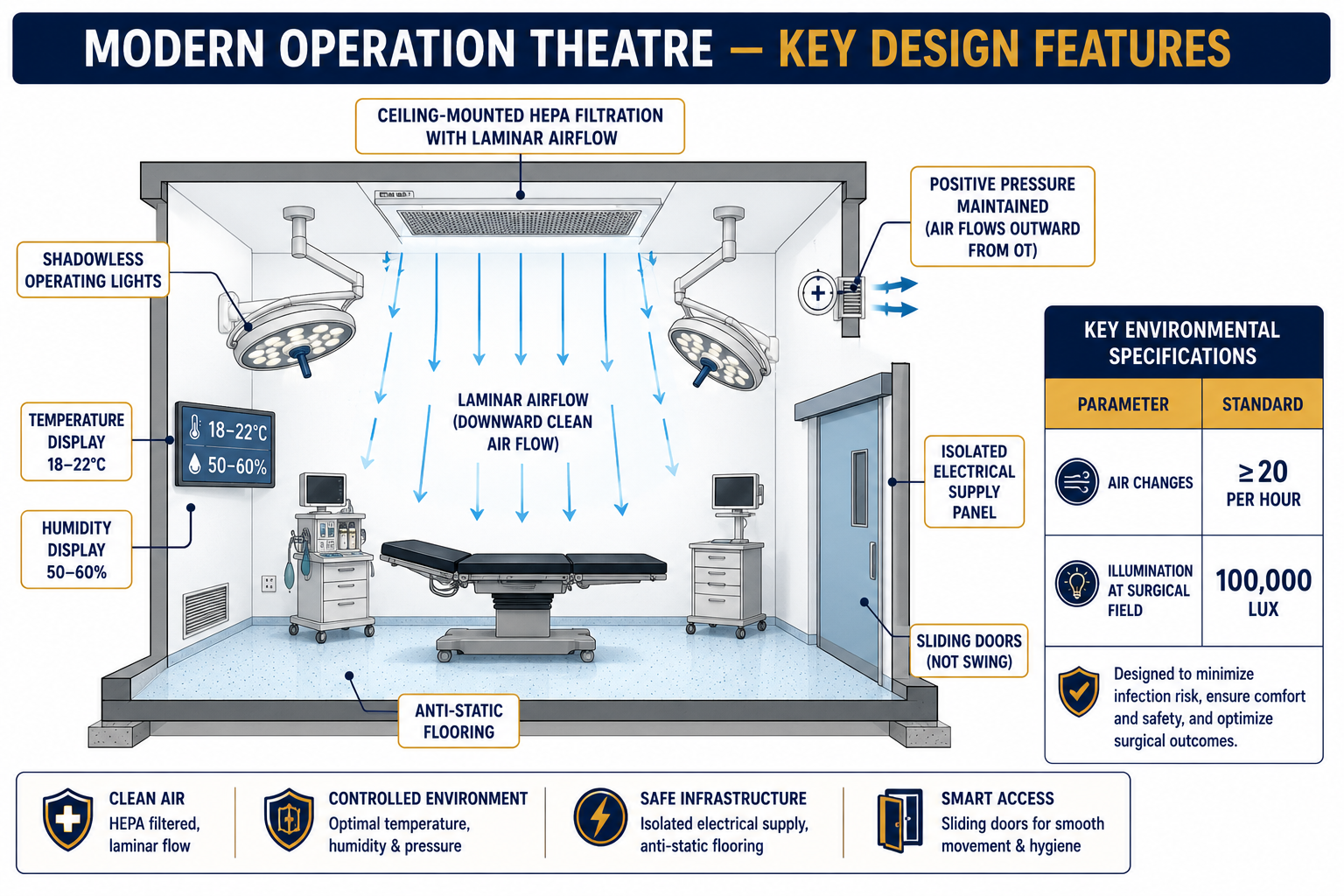
Key OT Features
- Laminar airflow: Positive pressure with HEPA filtration; ≥20 air changes/hour.
- Temperature: 18–22°C; humidity 50–60%.
- Lighting: Shadowless; 100,000 lux at operative field.
- Flooring: Anti-static, seamless.
- Traffic flow: Unidirectional — clean to dirty; no cross-traffic.
- Doors: Sliding (reduces turbulence); kept closed during surgery.
Bowel Preparation
►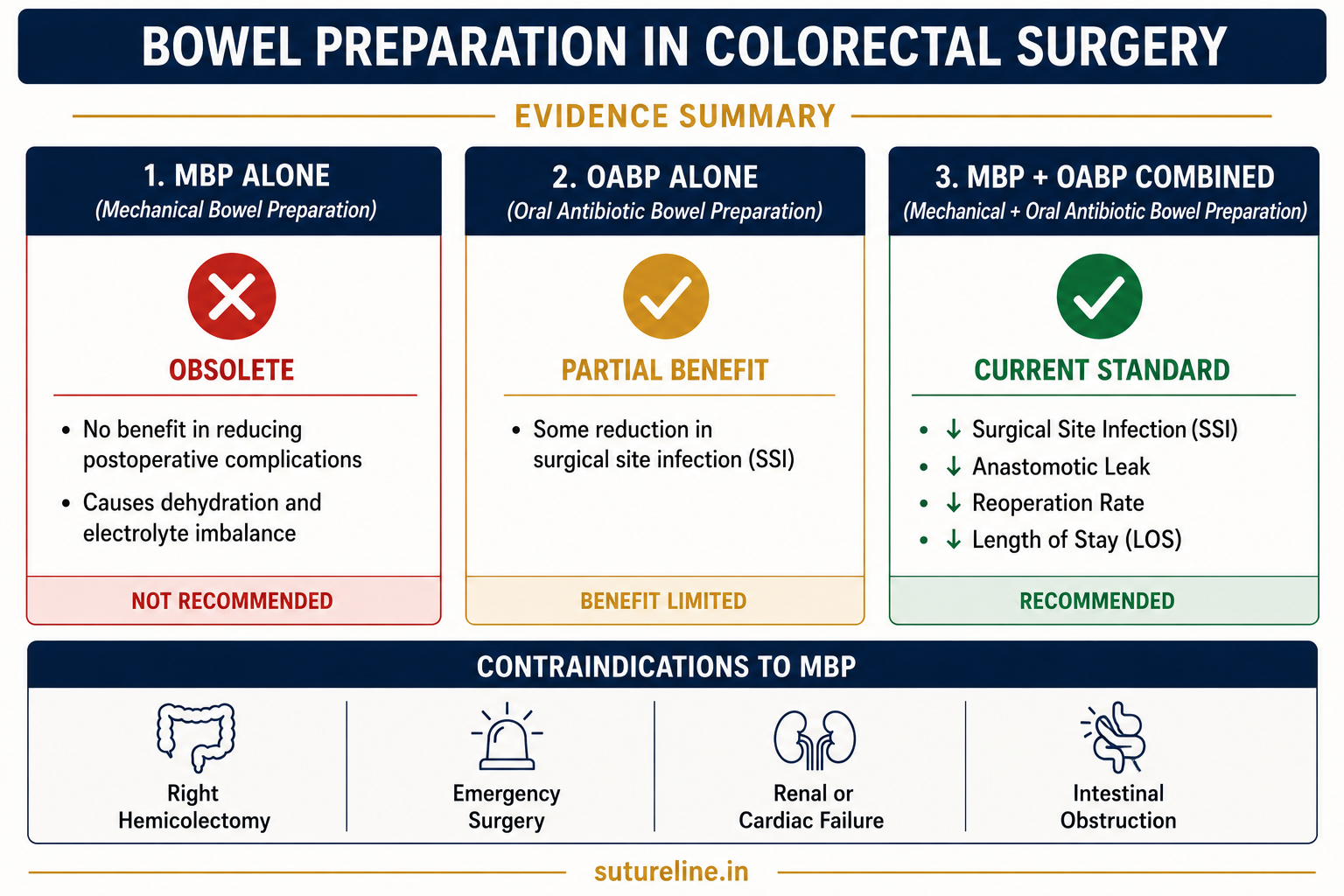
| Type | Agents | Evidence |
|---|---|---|
| MBP alone | PEG 4 L; sodium picosulfate | Obsolete — no benefit; may cause dehydration and electrolyte imbalance |
| OABP alone | Neomycin + Metronidazole (day before surgery) | Some benefit but limited; always add to systemic IV prophylaxis |
| MBP + OABP | Both combined | Current standard — significantly ↓ SSI, anastomotic leak, reoperation, LOS |
Practical Protocol — Elective Left-Sided Colorectal Surgery
- Low-residue diet 2–3 days before surgery.
- Day before: PEG solution until clear effluent; Neomycin 1 g + Metronidazole 1 g at 1 PM, 2 PM, 11 PM.
- Day of surgery: IV antibiotic prophylaxis 30–60 min before incision; clear fluids up to 2 h before anaesthesia (ERAS).
Acid–Base Disorders
►Normal Values
pH 7.35–7.45 | PaCO₂ 35–45 mmHg | HCO₃⁻ 22–26 mmol/L | Base Excess ±2 mmol/L. Compensation never fully normalises pH.
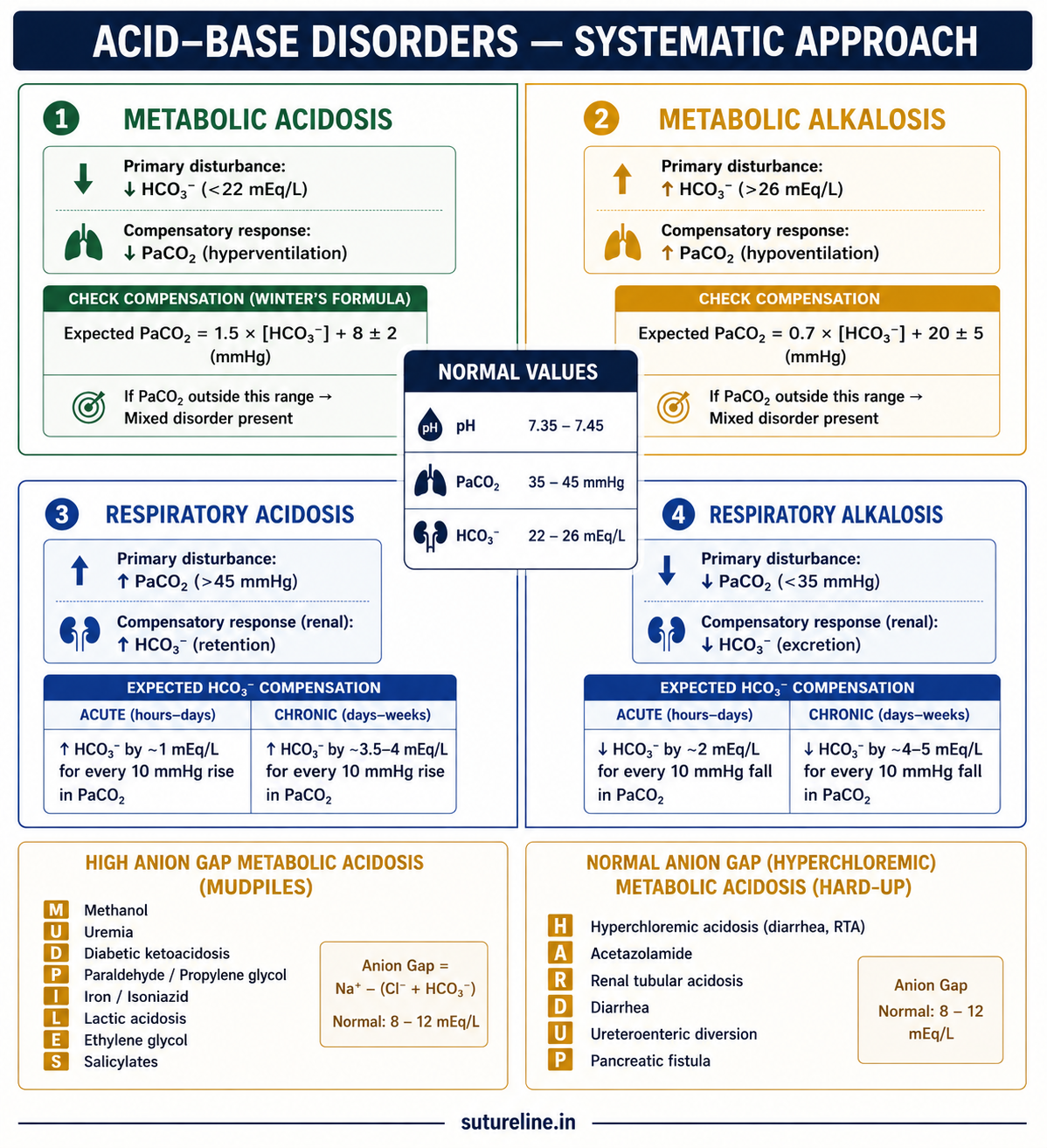
| Disorder | Primary Change | Compensation | Surgical Causes |
|---|---|---|---|
| Metabolic Acidosis | ↓ HCO₃⁻ | Hyperventilation → ↓ PaCO₂ (Winter's: PaCO₂ = 1.5×HCO₃ + 8 ± 2) | Shock, sepsis, DKA, renal failure, large-volume NS, lactic acidosis, pancreatic fistula |
| Metabolic Alkalosis | ↑ HCO₃⁻ | Hypoventilation → ↑ PaCO₂ (expected = 0.7×HCO₃ + 21 ± 2) | Prolonged vomiting (GOO), NG suction, diuretic excess, hypokalaemia |
| Respiratory Acidosis | ↑ PaCO₂ | Kidneys retain HCO₃⁻ (acute: ↑1 per 10↑PaCO₂; chronic: ↑3.5 per 10) | Post-op hypoventilation, opioid sedation, pneumothorax, flail chest, COPD |
| Respiratory Alkalosis | ↓ PaCO₂ | Kidneys excrete HCO₃⁻ (acute: ↓2 per 10↓PaCO₂; chronic: ↓5 per 10) | Pain, anxiety, fever, early sepsis, PE, over-ventilation |
Anion Gap in Metabolic Acidosis
AG = Na&spplus; − (Cl⁻ + HCO₃⁻). Normal = 8–12 mEq/L.
| High AG — MUDPILES | Normal AG — HARD-UP |
|---|---|
| Methanol, Uraemia, DKA, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethylene glycol, Salicylates | Hyperchloraemia (excess NS), Addison's, Renal tubular acidosis, Diarrhoea, Ureteroenteric diversion, Pancreatic fistula |
Hospital-Acquired Infections (HAI)
►Definition
Infections developing ≥48 hours after hospital admission, not incubating at time of admission, or within 30 days of an operative procedure. (Bailey & Love, 28th ed.)
Occur in 5–10% of hospitalised patients; up to 30% in ICU. Most common sites: urinary tract > surgical wound > respiratory tract > bloodstream.
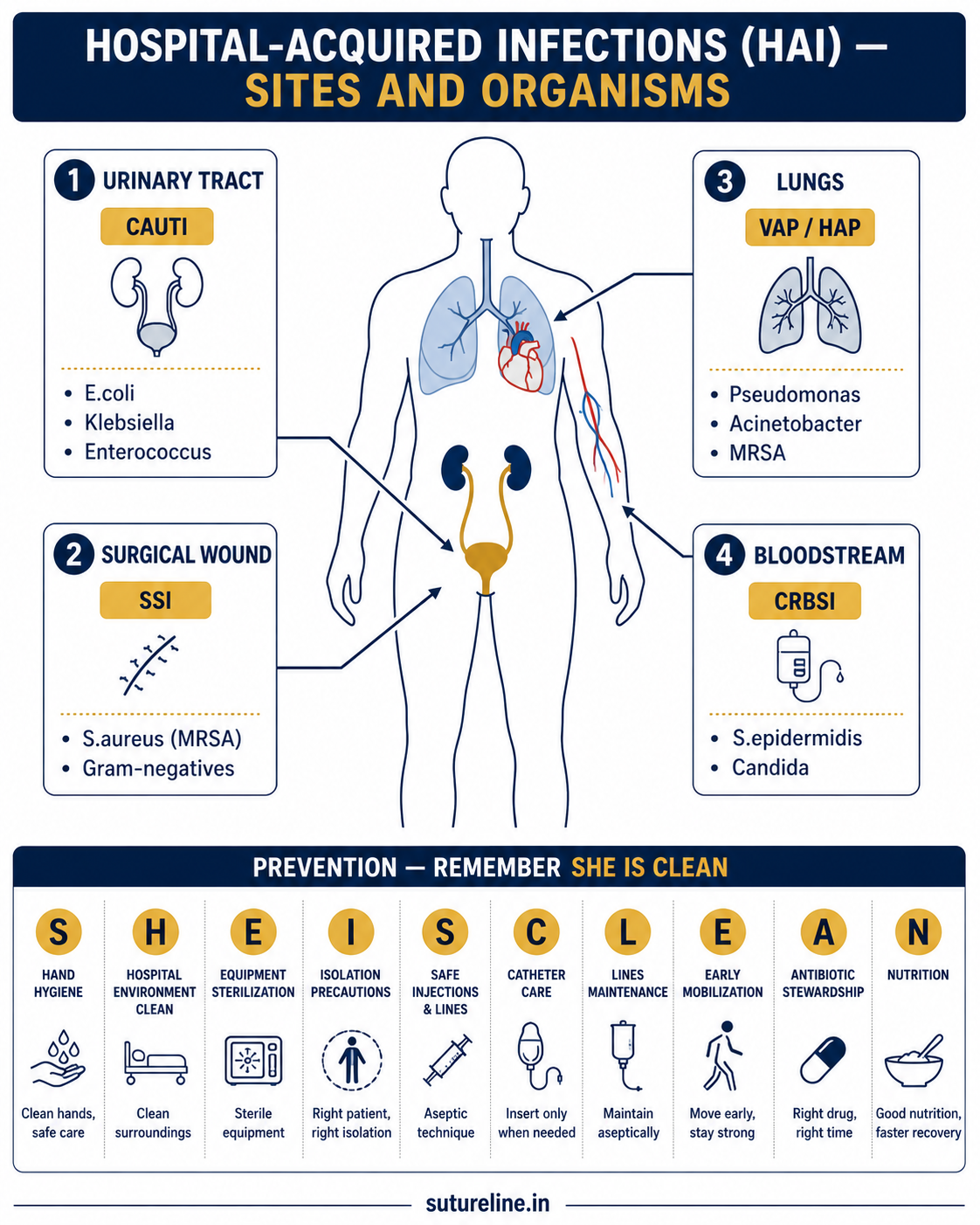
Prevention — “SHE IS CLEAN”
| Letter | Principle |
|---|---|
| S | Sterilisation of instruments |
| H | Hand hygiene — single most effective measure |
| E | Environmental cleaning |
| I | Isolation of cases |
| S | Surveillance and reporting |
| C | Catheter care |
| L | Line care |
| E | Education of staff |
| A | Antibiotic stewardship |
| N | Normothermia (perioperative) |
MRSA
►Definition
Staphylococcus aureus resistant to all β-lactam antibiotics via mecA gene → encodes PBP2a with low affinity for β-lactams. HA-MRSA = multidrug resistant (ICU, burns, postoperative). CA-MRSA = more virulent, less resistant; “spider-bite” lesions characteristic.
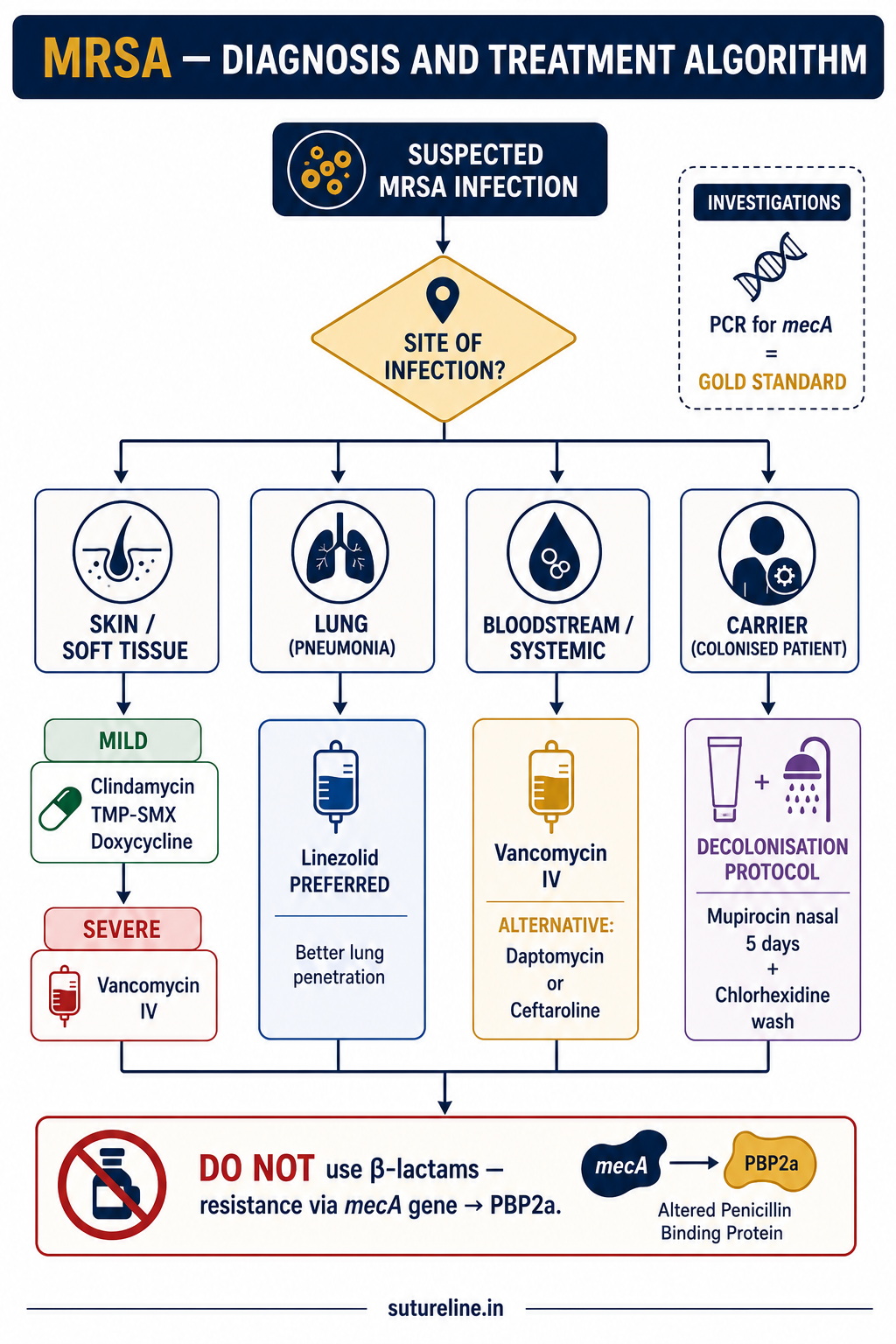
Treatment
| Infection Type | First-Line | Alternatives |
|---|---|---|
| Mild (skin/soft tissue) | Clindamycin, Doxycycline, TMP-SMX (CA-MRSA) | Linezolid (oral) |
| Severe/systemic | Vancomycin (IV) | Linezolid, Daptomycin, Teicoplanin, Ceftaroline |
| Pneumonia | Linezolid preferred | Vancomycin |
| Decolonisation | Mupirocin 2% nasal BD ×5 days + Chlorhexidine wash ×5 days | — |
Investigations: Culture + cefoxitin disc test; PCR for mecA gene = gold standard (same-day result).
Recent advances: Ceftaroline, ceftobiprole (anti-MRSA β-lactams); dalbavancin, oritavancin (long-acting lipoglycopeptides).
Surgical Site Infections (SSI)
►Definition & Classification
Infection at or near a surgical incision within 30 days (or 1 year if implant used) related to the surgery. Accounts for 20–30% of all HAIs.
- Superficial: Skin/subcutis
- Deep: Fascia/muscle
- Organ-space: Cavity or organ operated upon
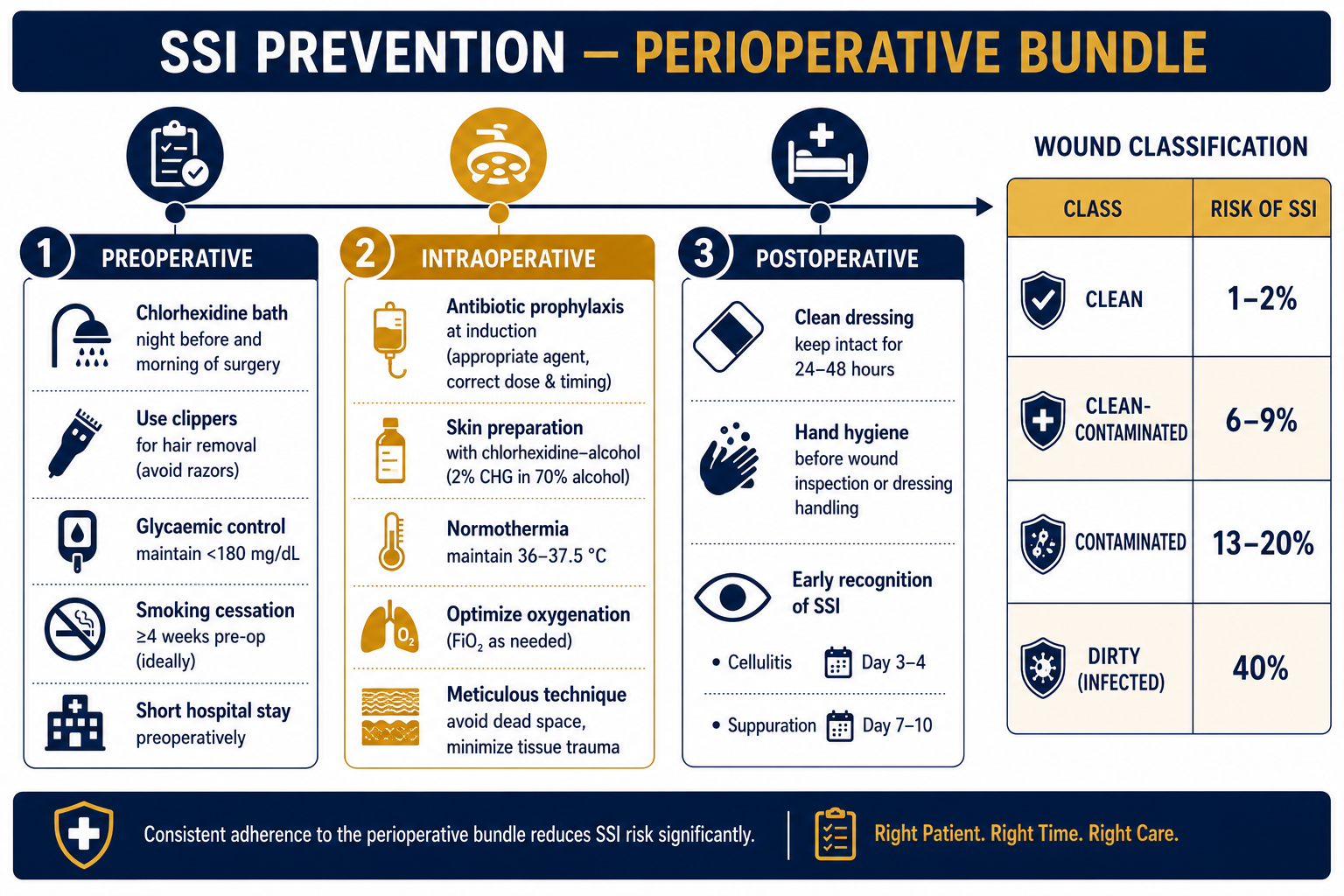
Wound Classification & SSI Rates
| Type | Description | Rate (no prophylaxis) | With prophylaxis |
|---|---|---|---|
| Clean | No viscus opened | 1–2% | 1–2% |
| Clean-contaminated | Viscus opened; minimal spillage | 6–9% | 3% |
| Contaminated | Gross spillage; inflamed viscus | 13–20% | 6% |
| Dirty | Pus; perforation; abscess | 40% | 7% |
Antibiotic Prophylaxis Principles
| Principle | Key Point |
|---|---|
| When | Clean with implant; clean-contaminated; contaminated |
| Timing | Single IV dose at induction of anaesthesia |
| Repeat | If >4 h duration or heavy blood loss |
| Stop | After skin closure — no postoperative doses |
| Choice | Cefazolin ± metronidazole (based on site and local flora) |
Management
Golden rule: Pus = Drain it. Remove sutures/clips → drain pus → debride necrotic tissue → antibiotics (empirical then per culture) → delayed primary closure (3–5 days) or secondary intention.
Ventilator-Associated Pneumonia (VAP)
►Definition
Pneumonia occurring ≥48 hours after endotracheal intubation. Most common HAI in ICU; mortality 30–50%. Pathogenesis: aspiration of oropharyngeal secretions around ETT cuff → lower respiratory tract inoculation.
Common organisms: Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae, MRSA.
VAP Prevention Bundle
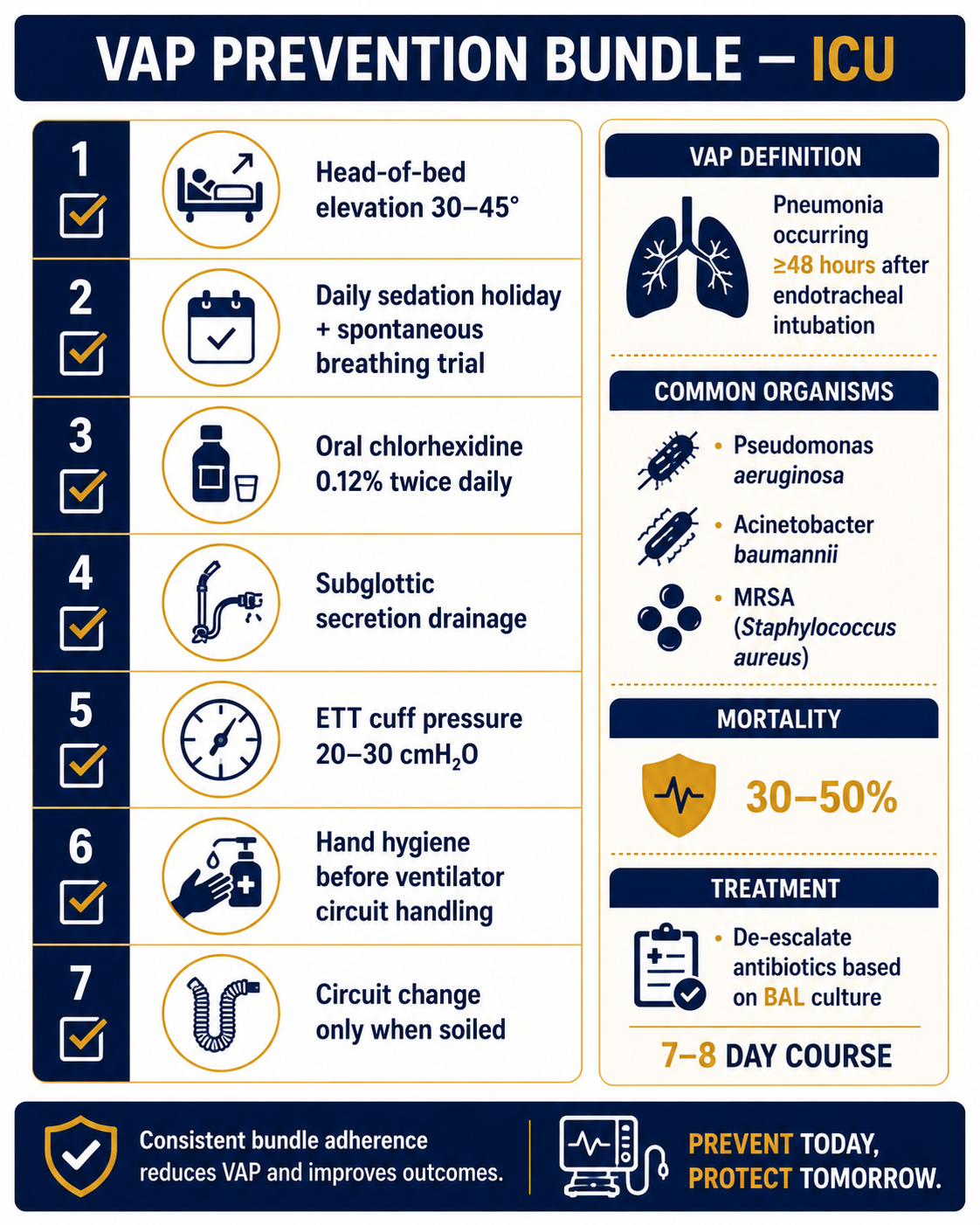
| Element | Detail |
|---|---|
| Head-of-bed elevation | 30–45° at all times (unless contraindicated) |
| Daily sedation holiday + SBT | Avoid prolonged ventilation; early weaning |
| Oral chlorhexidine hygiene | 0.12% twice daily; reduces oropharyngeal colonisation |
| Subglottic secretion drainage | Specialised ETT with subglottic suction port |
| ETT cuff pressure | 20–30 cmH₂O (prevents microaspiration) |
| Hand hygiene | Before and after all ventilator circuit handling |
Treatment: Empirical carbapenem or pip-tazo + MRSA cover; de-escalate per BAL culture (≥10⁴ CFU/mL); 7–8 day course.
Universal & Standard Precautions
►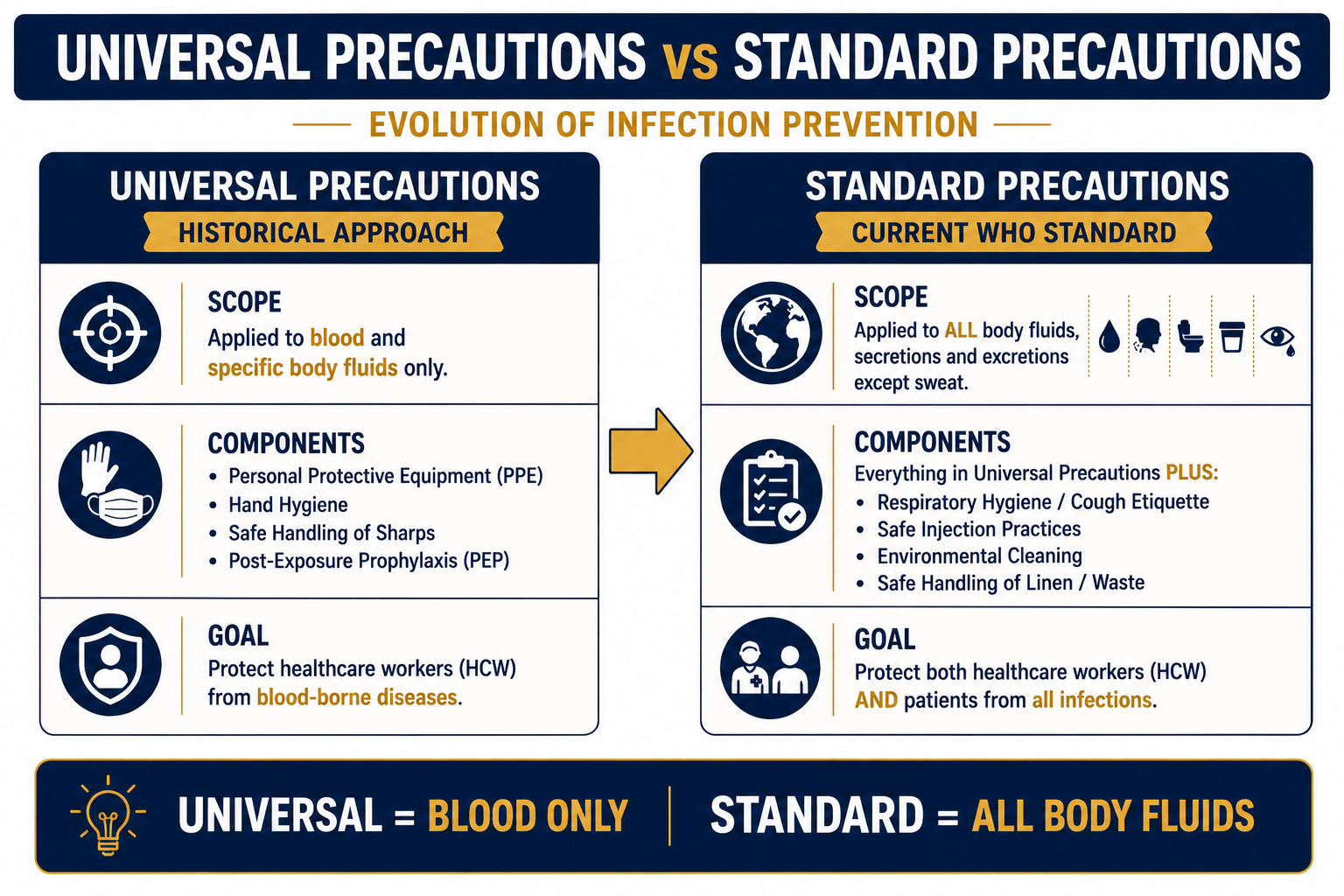
| Feature | Universal Precautions | Standard Precautions (Current) |
|---|---|---|
| Scope | Blood, semen, vaginal secretions, CSF, pleural/pericardial/peritoneal/synovial/amniotic fluid | All body fluids, secretions and excretions except sweat, whether or not they contain visible blood |
| Components | Hand hygiene, PPE, safe sharps, waste disposal, PEP after exposure | All Universal + respiratory hygiene, safe injection practices, environmental cleaning, linen management |
| Status | Precursor (replaced) | Current WHO standard |
| Goal | Protect HCWs from blood-borne diseases | Protect both HCWs and patients from all infections |
HIV and the Surgeon
►Risk of Transmission to Surgeon
| Exposure Type | Estimated HIV Risk |
|---|---|
| Needle-stick (hollow-bore needle) | ~0.3% |
| Mucocutaneous (splash to eye/mucosa) | ~0.09% |
| Intact skin exposure | Negligible |
| Scalpel injury | Up to 0.3–0.5% if deep |
HBV ~6–30% (without vaccination); HCV ~1.8%. Risk increases with: deep injury, visible blood on device, device used in artery/vein, high source viral load.
PEP Protocol
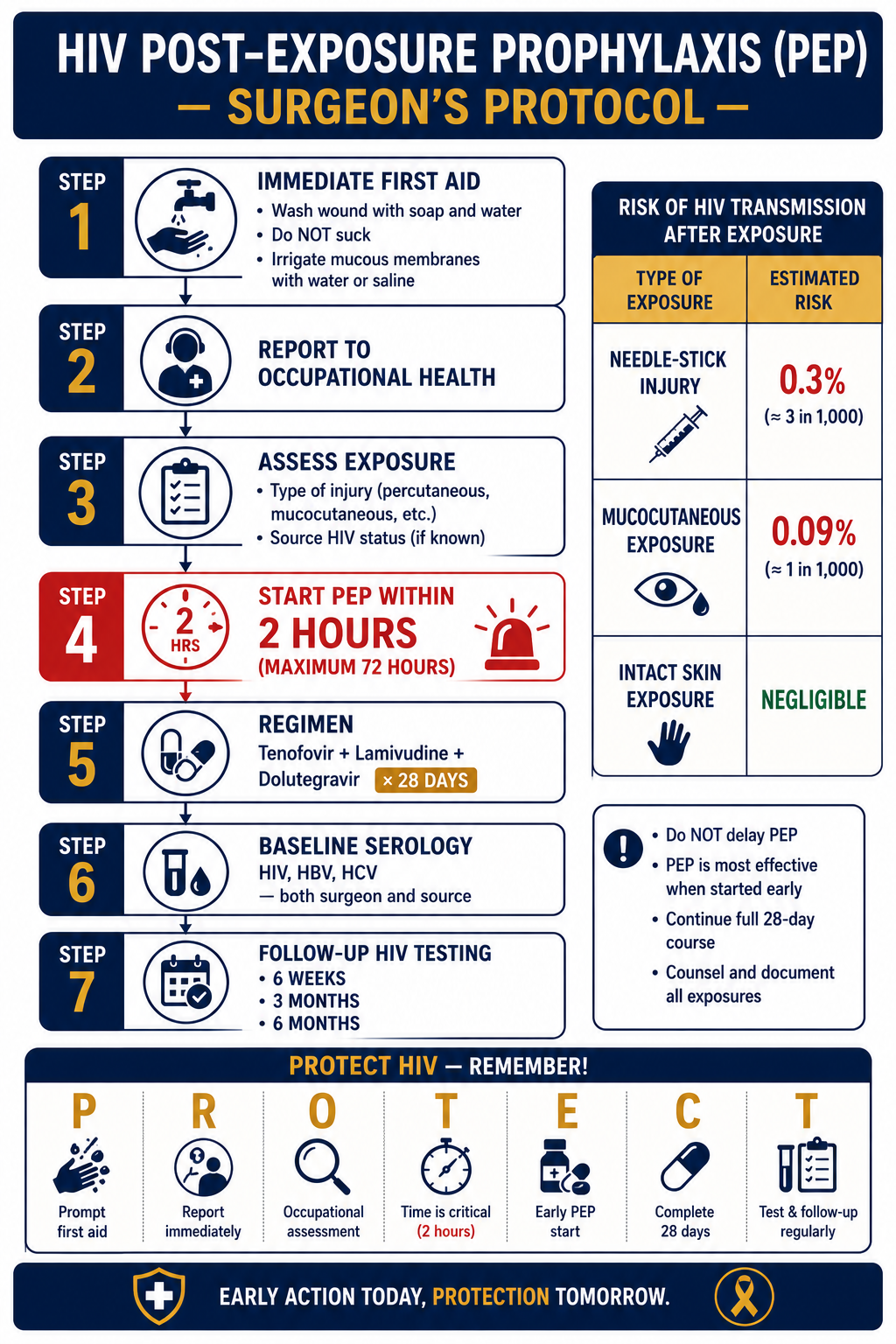
- Wash wound with soap and water immediately. Do not suck. Irrigate mucous membranes with saline/water.
- Report to occupational health immediately.
- Assess exposure — type of injury; source HIV status.
- Start PEP within 2 hours (max 72 hrs).
- 3-drug ART for 28 days: Tenofovir + Lamivudine (or Emtricitabine) + Dolutegravir.
- Baseline serology: HIV, HBV, HCV — both surgeon and source patient.
- Follow-up HIV testing at 6 weeks, 3 months, 6 months.
Ethical Aspects
| Aspect | Surgeon's Responsibility |
|---|---|
| Confidentiality | Patient's HIV status must remain strictly confidential |
| Informed consent | Discuss higher infection risk and wound complications preoperatively |
| Testing | Routine HIV testing of patients is unethical without consent |
| HIV-positive surgeon | May continue non–exposure-prone procedures; seek occupational health guidance for EPPs |