Fluids, Nutrition & Metabolism
From balanced crystalloids and GDFT targets to TPN complications and the MUST screening tool — the complete perioperative fluid and nutrition framework for MS and DNB exams.
Balanced Crystalloids vs Normal Saline
►
Definitions
Normal Saline (NS / 0.9% NaCl): 154 mEq/L each of Na&spplus; and Cl&supminus;; slightly hyperchloremic and hyperosmolar (~308 mOsm/L); pH ~5.5.
Balanced Crystalloids (BC): Ringer’s Lactate (RL) and Plasma-Lyte — electrolyte composition closer to plasma; chloride partially replaced by metabolisable buffers (lactate in RL; acetate + gluconate in Plasma-Lyte).
Composition Comparison
| Parameter | Balanced Crystalloids | Normal Saline | Plasma |
|---|---|---|---|
| Na&spplus; (mmol/L) | 130–140 | 154 | 140 |
| Cl&supminus; (mmol/L) | 98–110 | 154 | 103 |
| Buffer | Lactate (RL) / Acetate+Gluconate (PL) | None | Bicarbonate |
| pH | 6.5–7.4 | ~5.5 | 7.4 |
| Osmolarity (mOsm/L) | 273–294 | 308 | 295 |
| Volume distribution | 25% intravascular, 75% interstitial | Same | 100% intravascular |
Pathophysiology — Why NS Causes Problems
- High chloride load → hyperchloraemic metabolic acidosis via dilutional bicarbonate loss and direct renal tubular effects
- Renal vasoconstriction → reduced GFR → increased AKI risk in some settings
- Balanced crystalloids mitigate these effects — electrolyte profile closer to physiology
Clinical Evidence by Setting
| Setting | BC Advantage | Caution |
|---|---|---|
| Adult sepsis | Reduced 28-day mortality, lower AKI (SSC 2021 weak recommendation) | Low-quality evidence, more RCTs needed |
| Paediatric sepsis | Lower mortality, AKI, hyperchloraemia, shorter stay | — |
| DKA (adults) | Faster metabolic resolution, faster insulin weaning | Strong support for BC |
| TBI | Potentially harmful — BC may be hypotonic → cerebral oedema | Prefer NS in TBI |
| Critically ill (general) | Possibly lower composite mortality/AKI | Mixed, inconclusive overall |
Practical Recommendations
- Balanced crystalloids generally preferred in adult sepsis, paediatric sepsis, and DKA
- Normal saline remains appropriate in: TBI (cerebral oedema risk), alkalosis/hypochloraemia needing chloride load, hyperkalaemia (avoid lactate in RL)
- Choice should be individualized and context-specific
Colloids vs Crystalloids
►Definitions
Crystalloids: solutions of small molecules (electrolytes ± buffers) that pass freely through semipermeable membranes. Volume expands both intravascular and interstitial compartments.
Colloids: solutions of large-molecular-weight substances (proteins or polysaccharides) that stay in the intravascular space by exerting oncotic pressure.
Classification
- Crystalloids: Isotonic (0.9% NS, RL), Hypotonic (0.45% NS, D5W), Hypertonic (3% NS, 7.5% NS)
- Colloids — Natural: Albumin (4%, 5%, 20%), Fresh Frozen Plasma
- Colloids — Synthetic: Gelatins (Haemaccel, Gelofusine), Dextrans (Dextran-40, -70), HES (hydroxyethyl starch — withdrawn/restricted)
Volume Effect
- Crystalloids: 1L expands plasma volume by ~250–300 mL (rest redistributes to interstitium)
- Colloids: 1L expands plasma volume by ~800–1000 mL if endothelium is intact
- In capillary leak (sepsis, burns), colloids escape into interstitium — advantage is negated, oedema worsened
Key Trial Evidence
- SAFE trial (NEJM 2004): 4% albumin vs NS in 7,000 ICU patients — no overall mortality difference. Subgroup: TBI — albumin associated with increased mortality
- VISEP, 6S, CHEST trials: HES linked to increased AKI, increased RRT, possibly increased mortality — HES now restricted/avoided in sepsis and renal dysfunction
Comparison Table
| Feature | Crystalloids | Colloids |
|---|---|---|
| Oncotic pressure | Low | High |
| Volume expansion | Short-lived; ~25% remains intravascular | More sustained; ~80% intravascular (if intact endothelium) |
| Cost | Low | High (esp. albumin) |
| Allergy risk | Minimal | Yes (gelatins, dextrans) |
| Coagulopathy | Dilutional with large volumes | Dextrans, HES worsen coagulation |
| Renal toxicity | Rare (hyperchloraemia with NS) | HES — significant AKI risk |
Current Recommendations
- First line: balanced crystalloids for initial resuscitation in most surgical/ICU patients
- Normal saline: TBI, hyponatraemia, metabolic alkalosis needing chloride
- Albumin: adjunct in sepsis with hypoalbuminaemia after crystalloids; cirrhosis with large-volume paracentesis
- Synthetic colloids (HES, dextran, gelatin): avoid in sepsis, burns, renal dysfunction
Goal-Directed Fluid Therapy (GDFT)
►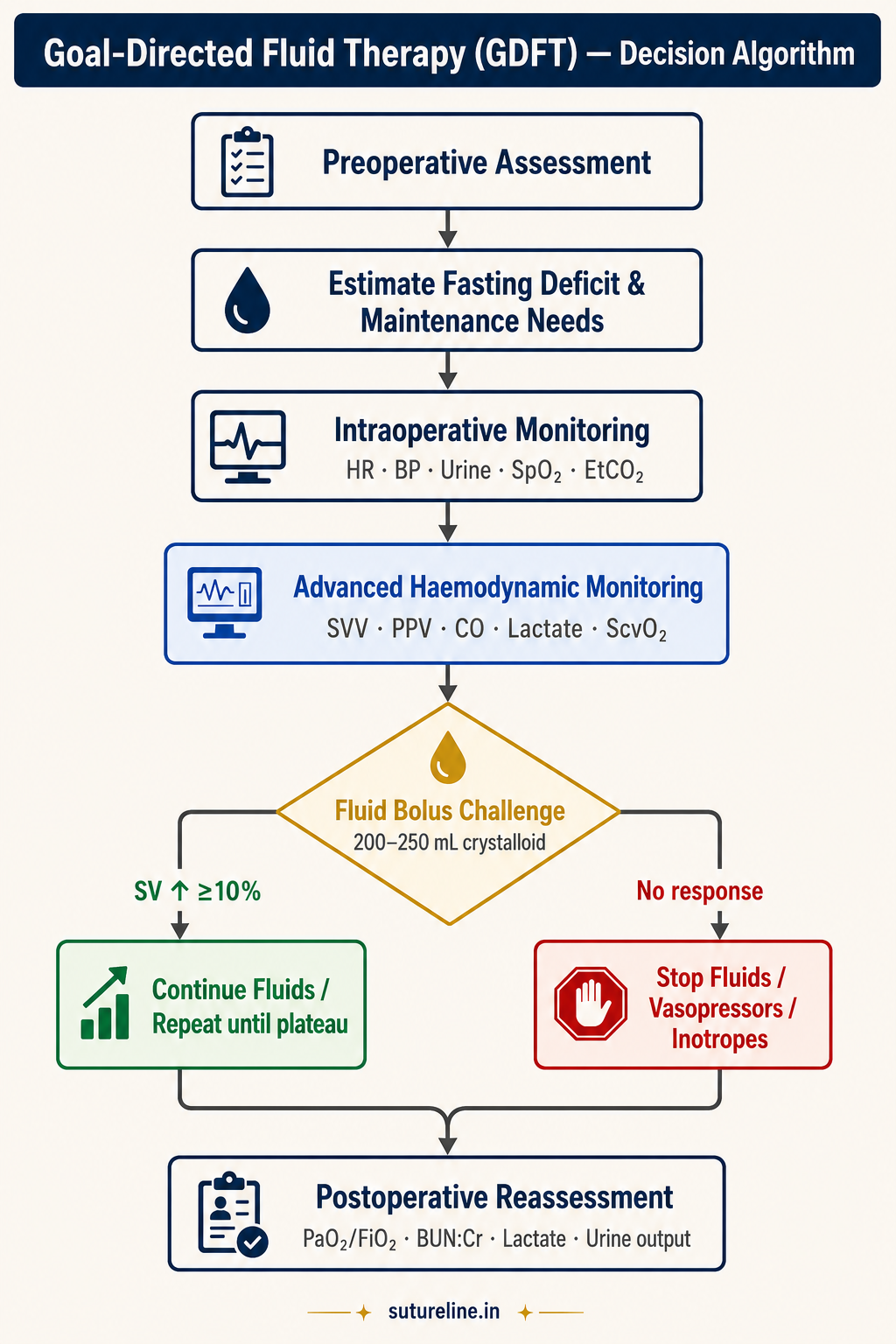
Definition
An individualised, dynamic approach to perioperative fluid administration guided by specific physiological targets (haemodynamic and perfusion parameters), aiming to optimise tissue oxygen delivery while avoiding both hypovolaemia and fluid overload.
Rationale
Traditional fixed-formula fluid therapy (body weight × estimated losses) leads to under-resuscitation (hypoperfusion, AKI) or overload (pulmonary oedema, impaired wound healing). GDFT uses real-time monitoring to titrate fluids to the patient’s physiological response.
GDFT Algorithm
Step 2: Assess response — measure SV, CO, SVV or PPV
Step 3a: Stroke volume rises ≥10% → fluid responsive → repeat bolus
Step 3b: No significant SV rise → fluid unresponsive → stop fluids, consider inotropes/vasopressors
Step 4: Reassess after each intervention
GDFT Monitoring Parameters
| Parameter | Target | Interpretation |
|---|---|---|
| Urine output | ≥0.5 mL/kg/hr | Adequate renal perfusion |
| MAP | ≥65 mmHg | Ensures organ perfusion |
| SVV (Stroke Volume Variation) | <10–12% after optimisation | >13% → fluid responsive |
| PPV (Pulse Pressure Variation) | <12% | >12% suggests preload responsiveness |
| Stroke volume | Optimise to plateau | No further rise after bolus = target met |
| Cardiac index | >2.2 L/min/m² | Adequate cardiac output |
| ScvO₂ | >70% | DO₂/VO₂ balance |
| Serum lactate | <2 mmol/L | Elevated → tissue hypoperfusion |
| BUN:Creatinine ratio | 10–20 normal | >20 hypovolaemia; <10 overload |
| PaO₂:FiO₂ | >300 | <300 suggests pulmonary overload/ARDS |
Devices Used
- Oesophageal Doppler (CardioQ) — non-invasive; standard for GDFT in UK
- LiDCO, PiCCO, FloTrac — minimally invasive cardiac output monitors
- Pulmonary artery catheter — gold standard but invasive; largely replaced
Evidence
OPTIMISE trial and multiple meta-analyses show GDFT reduces postoperative renal/pulmonary complications and hospital stay. Recommended by ERAS protocols. Effect on mortality less clear in lower-risk surgery.
IV Fluid Therapy in Adults — NICE CG174
►The 5 R’s of IV Fluid Therapy
- Resuscitation — restore intravascular volume in compromised patients
- Routine maintenance — meet daily basic fluid and electrolyte needs
- Replacement — correct existing deficits (dehydration, bleeding, losses)
- Redistribution — manage abnormal fluid shifts (oedema, third spacing)
- Reassessment — continuous monitoring and adjustment
Indications for Resuscitation
Any of: SBP <100 mmHg; HR >90/min; capillary refill >2 sec; RR >20/min; NEWS ≥5; positive passive leg raise response.
Resuscitation fluid: crystalloid (Na&spplus; 130–154 mmol/L); 500 mL bolus over <15 min; reassess after each bolus.
Routine Maintenance Prescription
Standard daily requirements:
- Water: 25–30 mL/kg/day
- Na&spplus;, K&spplus;, Cl&supminus;: ~1 mmol/kg/day each
- Glucose: 50–100 g/day (prevents ketosis)
Typical day-1 fluid: 0.18% NaCl + 4% dextrose + 27 mmol/L K&spplus;, ≤2.5 L/day.
Reduce to 20–25 mL/kg/day in: elderly, cardiac failure, renal disease, refeeding risk.
Common IV Fluids — Composition
| Fluid | Na&spplus; (mmol/L) | Cl&supminus; (mmol/L) | Use |
|---|---|---|---|
| 0.9% NaCl | 154 | 154 | Resuscitation (risk: hyperchloraemic acidosis) |
| Hartmann’s / RL | 131 | 111 | Balanced resuscitation (preferred) |
| 5% Dextrose | 0 | 0 | Free water replacement (not resuscitation) |
| 4% Dextrose + 0.18% NaCl | 30 | 30 | Routine maintenance |
Complications of IV Fluid Therapy
| Complication | Definition | Time Frame |
|---|---|---|
| Hypovolaemia | Clinical dehydration, ↑urea/Cr, low urine output | During therapy |
| Pulmonary oedema | Breathlessness, X-ray infiltrates | During / ≤6h post-IVF |
| Hyponatraemia | Na&spplus; <130 mmol/L | ≤24h post-IVF |
| Hypernatraemia | Na&spplus; ≥155 mmol/L | ≤24h post-IVF |
| Hypo/hyperkalaemia | K&spplus; <3.0 or >5.5 mmol/L | ≤24h post-IVF |
| Peripheral oedema | Pitting oedema without cardiac/renal cause | ≤24h post-IVF |
Artificial Nutritional Support
►Introduction & Indications
Adequate nutrition is vital for postoperative recovery and wound healing. Artificial nutritional support is indicated when oral intake is inadequate for >5 days, or earlier in malnourished patients.
Commonly required in: major head/neck/GI surgery (oesophagectomy, gastrectomy, Whipple’s), severe trauma/burns, sepsis, neurological impairment, prolonged ileus, high-output fistulae.
Routes — Enteral vs Parenteral
| Feature | Enteral Nutrition | Parenteral Nutrition |
|---|---|---|
| Route | GI tract | Intravenous (peripheral or central) |
| Gut integrity | Maintains mucosal integrity and GALT | Mucosal atrophy, bacterial translocation risk |
| Infection risk | Lower | Higher (catheter-related sepsis) |
| Cost | Cheaper | Expensive |
| Indication | When gut is functional | When gut unusable or contraindicated |
| Main complications | Aspiration, diarrhoea, tube issues | Metabolic, hepatic, catheter-related |
Enteral Nutrition
►Definition
Delivery of nutrients directly into the GI tract through oral, gastric, or post-pyloric routes, when normal oral intake is inadequate but the gut is functional.
Types by Nutrient Composition
- Polymeric: intact protein, polysaccharides, long-chain TG — requires normal digestion; standard for most patients
- Elemental/monomeric: amino acids, monosaccharides, MCT — for malabsorption, short bowel, pancreatitis
- Semi-elemental (oligomeric): peptides, oligosaccharides, MCT — intermediate absorption
- Disease-specific: renal (low protein/K), hepatic (BCAA-enriched), pulmonary (high fat/low CHO), diabetic (low GI, fibre-added)
Access Routes by Duration
| Route | Duration | Indication |
|---|---|---|
| Nasogastric (NG) | ≤4–6 weeks | Short-term; intact gag reflex; most common |
| Nasojejunal (NJ) | ≤4–6 weeks | High aspiration risk; acute pancreatitis |
| PEG (Percutaneous Endoscopic Gastrostomy) | >4–6 weeks | Long-term; intact gastric emptying; neurological conditions |
| RIG (Radiologically Inserted Gastrostomy) | >4–6 weeks | Endoscopy not feasible |
| Jejunostomy (PEJ / surgical) | Long-term | Gastroparesis; gastric outlet obstruction; post-oesophagectomy |
Advantages of Enteral over Parenteral
- Physiological: preserves gut mucosal integrity; maintains GALT; decreases bacterial translocation; stimulates bile flow and pancreatic secretions
- Clinical: lower infection incidence; better glycaemic control; early EN reduces post-op ileus and improves wound healing
- Practical: cheaper; easier administration; fewer metabolic complications
Complications
| Category | Complications |
|---|---|
| Mechanical | Malposition, kinking, blockage, dislodgement; nasal/oesophageal ulceration, sinusitis; aspiration pneumonia |
| Gastrointestinal | Nausea, vomiting, distension; diarrhoea (osmotic/rapid infusion); constipation; GI bleeding |
| Metabolic | Electrolyte imbalance; hyperglycaemia; refeeding syndrome; dehydration or overload |
| Infective | Sinusitis, otitis (nasal tubes); peristomal infection (PEG/jejunostomy); peritonitis (leak) |
Contraindications
Absolute: intestinal obstruction (mechanical or paralytic ileus); severe mesenteric ischaemia; peritonitis or intra-abdominal sepsis; severe GI haemorrhage; inability to access GI tract safely.
Relative: high aspiration risk with unprotected airway; haemodynamic instability on high-dose vasopressors (bowel ischaemia risk); severe uncontrolled diarrhoea; severe pancreatitis (NJ feeding often still feasible).
Parenteral Nutrition (PN)
►Definition
Administration of nutrients intravenously, bypassing the GI tract, to provide substrates for energy, growth, and tissue repair when enteral feeding is not possible.
Types
- Partial PN (PPN): supplies part of daily requirements; peripheral access acceptable; lower osmolarity (<900 mOsm/L)
- Total PN (TPN): full caloric/nutritional requirements; requires central venous access (high osmolarity); contains dextrose + amino acids + lipids + electrolytes + vitamins + trace elements
Access Routes
| Route | Duration | Comment |
|---|---|---|
| Central Venous Catheter (CVC) | Long-term | Preferred; reduces thrombophlebitis |
| PICC line | Weeks–months | Inserted via basilic/cephalic vein; good for home TPN |
| Peripheral line | <14 days | Low osmolarity feeds only (<900 mOsm/L) |
| Hickman / Implanted port | >3 months | Long-term home TPN; tunnelled |
Indications
- Intestinal obstruction, severe short bowel syndrome, high-output enterocutaneous fistulae
- Severe pancreatitis where EN not tolerated; intractable vomiting/diarrhoea
- Perioperative: preoperative severe malnutrition; prolonged postoperative NPO after major GI surgery
- Critical illness: severe trauma, burns, sepsis where EN not feasible
- Oncology: malignant bowel obstruction, radiation enteritis
Complications
| Type | Examples |
|---|---|
| Insertion-related | Pneumothorax (0.5–1%; subclavian route), arterial puncture, misplacement — confirm position on CXR |
| Line-related | Catheter-related bloodstream infection (CRBSI) up to 15%; thrombosis (SVC occlusion/PE); line blockage |
| Metabolic | Hyperglycaemia (most common); refeeding syndrome; electrolyte derangements (Na, K, Mg, PO₄) |
| Hepatic (IFALD) | Fatty liver → fibrosis → cirrhosis (~25% incidence in long-term TPN; especially children) |
| Metabolic bone disease | Osteoporosis/osteomalacia; supplement Ca²&spplus;, PO₄, Vit D |
Risk factors: BMI <16; weight loss >15% in 3–6 months; no intake >10 days; low baseline K&spplus;/Mg/PO₄; alcoholism.
Prevention: start at 10 kcal/kg/day; increase slowly over 4–7 days; supplement thiamine, vitamins, trace elements before and during refeeding; monitor electrolytes daily.
Caloric & Protein Requirements
►Metabolic Phases After Surgery
| Phase | Duration | State | Features |
|---|---|---|---|
| Ebb phase | 0–24 hrs | ↓ Metabolism | ↓ O₂ consumption, ↓ energy expenditure, ↓ body temperature |
| Flow phase | 2–10 days | ↑ Catabolism | ↑ cortisol, ↑ catecholamines, ↑ gluconeogenesis, ↑ protein breakdown |
| Anabolic phase | After 7–10 days | ↑ Protein synthesis | Tissue repair, positive nitrogen balance |
Energy Requirements
Total Energy Requirement (TER) = BEE × (stress factor + activity factor)
| Condition | Stress Factor | Approx. kcal/kg/day |
|---|---|---|
| Post-op elective surgery | 1.1–1.2 | 25–30 |
| Moderate infection/trauma | 1.3–1.5 | 30–35 |
| Sepsis / major burns / multiple trauma | 1.5–2.0 | 35–45 |
| Severe burns (>40% BSA) | 2.0–2.5 | Up to 50 |
Protein Requirements
| Condition | Protein (g/kg/day) |
|---|---|
| Normal adult | 0.8–1.0 |
| Post-operative mild stress | 1.0–1.2 |
| Moderate stress (infection/trauma) | 1.3–1.5 |
| Severe stress / burns / sepsis | 1.5–2.0 |
| Protein-losing conditions | Up to 2.5 |
Macronutrient Summary
| Parameter | Normal | Post-op mild | Severe stress/sepsis |
|---|---|---|---|
| Calories (kcal/kg) | 25 | 30–35 | 40–50 |
| Protein (g/kg) | 1.0 | 1.2–1.5 | 2.0 |
| Carbohydrates (g/kg) | 3–4 | 4–5 | 5–6 |
| Fat (g/kg) | 1.0 | 1–2 | 2.0 |
| Water (mL/kg) | 30–35 | 30–40 | 40–50 |
Nitrogen balance: goal is positive nitrogen balance (nitrogen in > nitrogen out). Nitrogen intake (g) = Protein intake (g) ÷ 6.25.
Nutritional Assessment & MUST Tool
►ABCD Approach to Nutritional Assessment
A — Anthropometry
- BMI = weight (kg) ÷ height² (m²)
- MUAC (Mid-Upper Arm Circumference)
- TSF (Triceps Skinfold Thickness)
- MAMC (Mid-Arm Muscle Circumference) = MUAC − (3.14 × TSF)
- Caveat: anthropometry is altered by fluid shifts in critically ill patients
B — Biochemistry
- Albumin: falls in malnutrition/inflammation; not reliable acutely (half-life 20 days)
- Prealbumin: shorter half-life (2 days) — better acute marker
- CRP, WBC: inflammation markers
- Electrolytes (Na&spplus;, K&spplus;, Mg, PO₄): assess refeeding risk
C — Clinical evaluation
- Symptoms: nausea, vomiting, dysphagia, early satiety, diarrhoea
- Past history: malignancy, IBD, liver disease, stroke, Parkinson’s
- Malabsorptive states: short bowel, high-output stoma, enterocutaneous fistula, pancreatic insufficiency
D — Dietary assessment
- Diet diary or 24-hour dietary recall
- Compare to requirement (25–35 kcal/kg lean body weight)
- Recent or anticipated decreased intake >5 days → initiate nutritional support
MUST Tool (Malnutrition Universal Screening Tool)
| Parameter | Score 0 | Score 1 | Score 2 |
|---|---|---|---|
| BMI (kg/m²) | ≥20 | 18.5–20 | <18.5 |
| Weight loss (3–6 mo) | ≤5% | 5–10% | >10% |
| Acute disease effect | – | – | Add 2 if likely no intake ≥5 days |
| Total Score | Risk | Action |
|---|---|---|
| 0 | Low | Routine care; weekly hospital reassessment |
| 1 | Medium | Observe; document intake for 3 days |
| ≥2 | High | Dietician referral; initiate nutritional support |
Follow-up Frequency
- Hospital: weekly
- Care homes: monthly
- Community: yearly (age >75 years)