Devices, Energy & Technology
From monopolar diathermy to harmonic scalpel, circular staplers to bioengineered scaffolds — the full technology toolkit of modern surgery, with selection algorithms and exam-focused comparisons.
Energy Devices in Surgery
►
Definition
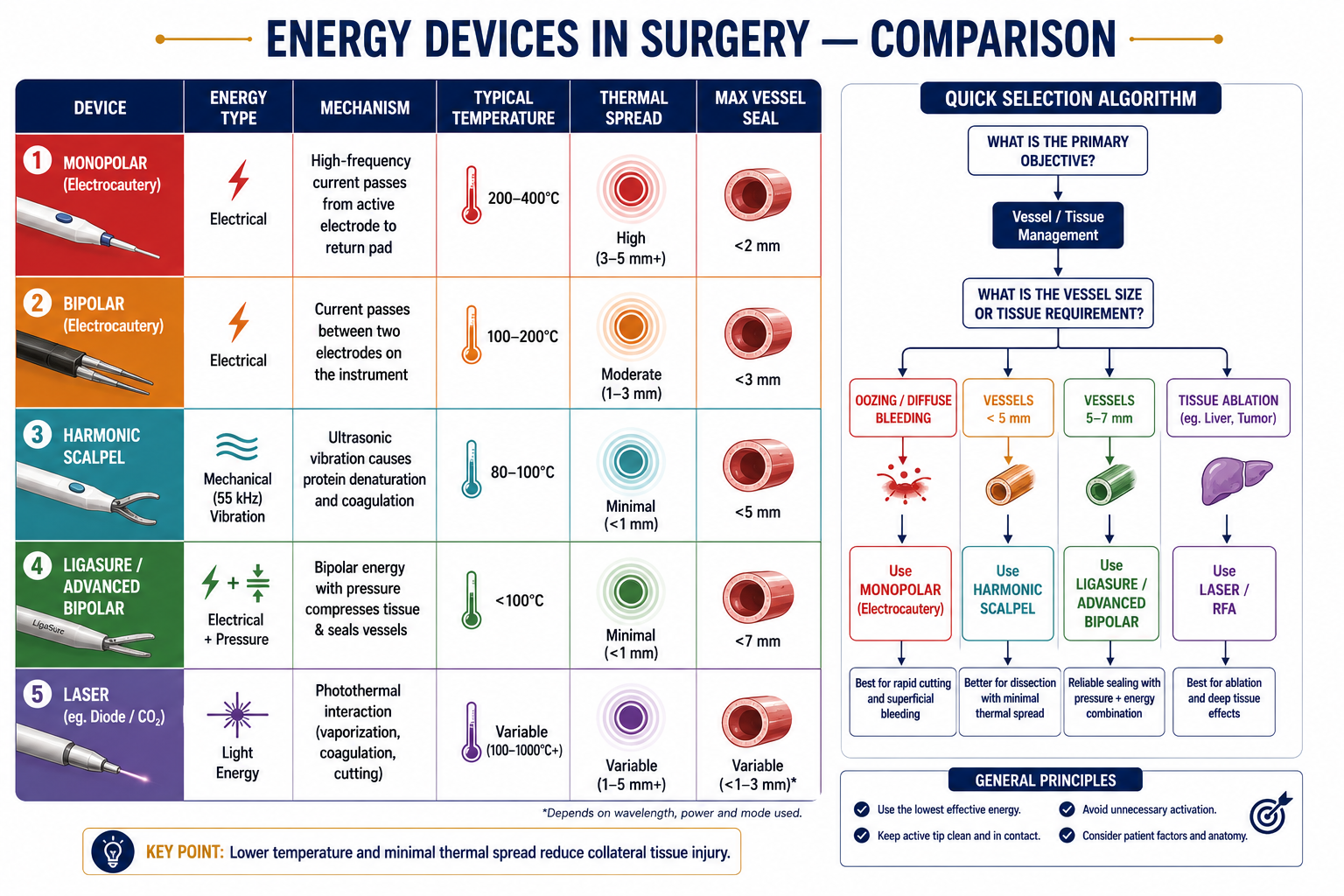
Energy devices in surgery are instruments that utilise various forms of energy — electrical, mechanical, ultrasonic, or thermal — to cut, coagulate, seal, or ablate tissue, thereby reducing blood loss and operative time.
Classification
| Energy Type | Device Examples | Mechanism | Tissue Effect |
|---|---|---|---|
| Electrical — Monopolar | Standard diathermy | HF alternating current → patient → return pad | Cutting, coagulation |
| Electrical — Bipolar | Bipolar forceps | Current confined between two jaw tips | Precise coagulation |
| Advanced Bipolar | LigaSure, Enseal, Caiman, Marseal | Bipolar + pressure + impedance feedback | Vessel sealing ≤7 mm |
| Ultrasonic | Harmonic Scalpel, Ultracision | 55 kHz vibration → protein denaturation | Cut + coagulate at ≤100°C |
| Hybrid / Combined | Thunderbeat, Sonicision | Ultrasonic + bipolar in one instrument | Rapid dissection + sealing |
| Laser | CO&sub2;, Nd:YAG, KTP, Diode | Light energy → thermal effect | Vaporisation, coagulation |
| Radiofrequency | RFA devices | 400–500 kHz alternating current → ionic agitation | Coagulative necrosis (ablation) |
| Argon Plasma (APC) | Argon beam coagulator | Ionised argon gas conducts monopolar current | Non-contact superficial coagulation |
| Microwave / Plasma | PlasmaJet, microwave ablation | EM radiation / ionised gas jet | Coagulation, tissue vaporisation |
Key Devices — Principles
1. Harmonic Scalpel (Ultrasonic)
- Converts electrical → mechanical energy at 55,000 Hz vibration
- Causes protein denaturation and vessel sealing without current passing through tissue
- Temperature: 80–100°C (much lower than electrocautery)
- Advantages: Minimal smoke, less thermal damage, effective vessel sealing ≤5 mm
2. Advanced Bipolar Devices (LigaSure, Enseal)
- Use pressure + controlled bipolar energy
- Denature collagen and elastin forming a permanent tissue seal
- Impedance feedback mechanism stops energy delivery when seal is complete
- Seals vessels up to 7 mm
3. Laser Surgery
- CO&sub2; laser: superficial vaporisation (laryngeal, skin, ENT)
- Nd:YAG: deep penetration (GI endoscopy, tumour ablation)
- KTP: photocoagulation (prostate, ENT)
- Hazards: eye injury, smoke plume, fire risk
4. Argon Plasma Coagulation (APC)
- Non-contact modality — ionised argon gas conducts current without touching tissue
- Uniform superficial coagulation, especially in endoscopic and hepatic surgery
- Limitation: poor depth control → risk of perforation
5. Radiofrequency Ablation (RFA)
- Used for: hepatic, renal, thyroid, and pulmonary tumours
- Generates ionic agitation and localised heat → coagulative necrosis
Comparison Table
| Feature | Monopolar | Bipolar | Harmonic | LigaSure |
|---|---|---|---|---|
| Energy Type | Electric | Electric | Mechanical | Electric |
| Tissue Temp (°C) | 200–400 | 100–200 | 80–100 | <100 |
| Cut + Coagulate | Yes | Limited | Yes | Yes |
| Smoke | High | Moderate | Low | Low |
| Thermal Spread | High | Moderate | Minimal | Minimal |
| Vessel Seal (mm) | <2 | <3 | <5 | <7 |
Device Selection Algorithm
Minor oozing / small vessels → Monopolar / bipolar
Up to 5 mm vessels → Harmonic scalpel
Up to 7 mm vessels → Advanced bipolar (LigaSure)
Rapid cut + seal needed → Hybrid device (Thunderbeat)
Tumour ablation → RFA / microwave / cryo
Proximity to vital structures:
Near ureter, nerves → Low-thermal devices (ultrasonic, advanced bipolar with feedback); avoid monopolar
MIS / robotic field:
Prefer instruments that reduce exchanges; use multi-function devices sized for laparoscopic use
Safety & Precautions
- Proper placement of return electrode pad (monopolar)
- Avoid flammable agents near monopolar (oxygen, alcohol-based prep)
- Smoke evacuation — surgical plume contains toxins and aerosolised viral/bacterial particles
- Beware insulation failure and capacitive coupling in laparoscopy
- Periodic calibration and staff training essential
Recent Advances
- Thunderbeat: Combines ultrasonic + bipolar energy in a single instrument for rapid dissection with reliable sealing
- CoolSeal: Reduced thermal spread sealing device
- Smart impedance feedback: AI-integrated real-time energy modulation; stops delivery at optimal seal endpoint
- Caiman long-jaw design: More uniform energy delivery, improved burst pressure, reduced thermal spread
- Plasma/tissue-plasma cutting devices: Increasing use in robotic settings for controlled vaporisation
Diathermy & Electrosurgery
►Principle
Diathermy uses high-frequency alternating current (300 kHz – 3 MHz) to generate heat at the electrode–tissue interface. At these frequencies, current does not stimulate nerve or muscle (no electrocution), but generates enough thermal energy to cut or coagulate.
Types
Monopolar Diathermy
- Current flows from active electrode → through patient's body → return (dispersive) pad
- Modes: Cut (continuous waveform, rapid heating → vaporises cells) and Coagulate (interrupted waveform, slower heating → protein denaturation)
- Blend mode: mixture of cut and coag waveforms
- Contraindications: pacemakers, implanted metallic devices, crossing vital structures
Bipolar Diathermy
- Current confined between two tips of forceps — no return pad needed
- Suitable for precise coagulation of small vessels, neurosurgery, and ophthalmic work
- Disadvantage: cannot cut, slower than monopolar, limited to small tissue volumes
Complications of Diathermy
| Complication | Mechanism | Prevention |
|---|---|---|
| Pad site burns | High current density at return pad if pad is poorly applied or partially detached | Proper pad placement, adequate contact area |
| Stray current burns | Current seeking alternative earth paths — through metal cannulas, ECG electrodes | Isolate patient from earth; use bipolar in sensitive areas |
| Capacitive coupling | Current induced in adjacent conductor (e.g., metal cannula in laparoscopy) without direct contact | All-metal or all-plastic trocar systems; avoid hybrid |
| Insulation failure | Defective insulation on laparoscopic instrument allows current escape to bowel | Inspect insulation before use; active electrode monitoring |
| Pacemaker interference | Monopolar current may trigger or inhibit pacemaker | Use bipolar; keep return pad distant from pacemaker; cardiology standby |
| Diathermy fires | High current + flammable agent (O&sub2;, alcohol prep) | Allow alcohol prep to dry; avoid open O&sub2; near field |
Staplers in Surgery
►
Definition
A surgical stapler is a mechanical device that applies metallic or absorbable staples to close or join tissues, offering a faster and more consistent alternative to manual suturing.
Basic Components
- Handle/Trigger — activates the stapling mechanism
- Cartridge — contains the staples (replaceable/reloadable)
- Anvil — shapes and bends the staples into a B-shape
- Knife blade (in cutting staplers) — divides tissue between staple rows simultaneously
Staple Materials
- Metallic: Titanium (commonest), stainless steel
- Absorbable: Polyglycolic acid (PGA), Polylactide (PLA) — useful where imaging interference is a concern
Types of Staplers
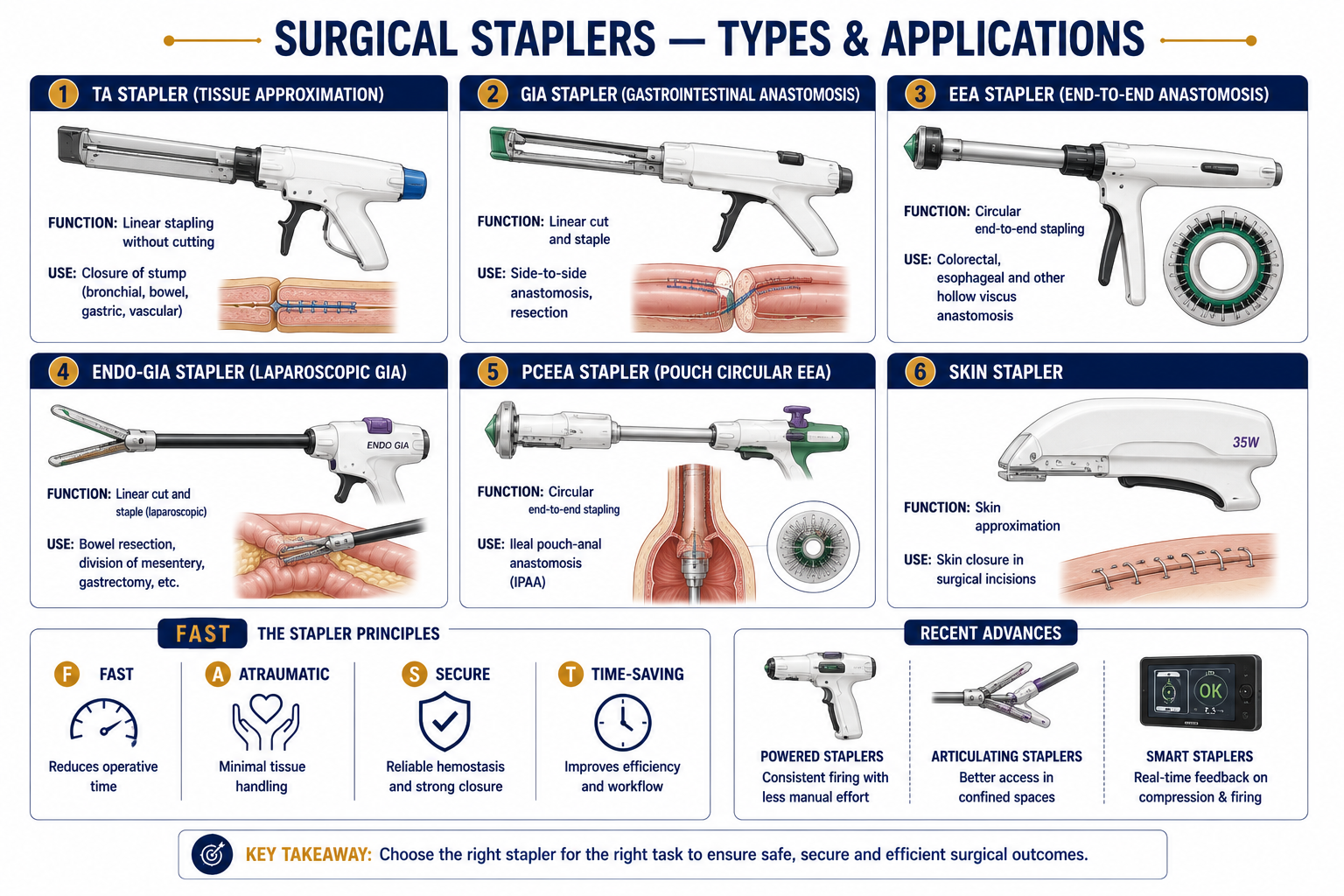
| Type | Full Form | Function | Common Use |
|---|---|---|---|
| TA | ThoracoAbdominal stapler | Places 2–3 linear rows, no cutting | Bowel/bronchial stump closure |
| GIA | GastrointestinalAnastomosis stapler | Two double rows + cuts between them | Side-to-side bowel anastomosis; bowel resection |
| EEA | End-to-End Anastomosis stapler | Circular stapler — cuts and staples simultaneously | Oesophageal, gastric, colorectal anastomosis |
| ILS | IntraLuminal Stapler | Similar to EEA (circular) | Low anterior resection; oesophagogastric anastomosis |
| PCEEA | Premium Circular End-to-End Anastomosis | Improved circular compression and cutting | Ileal pouch–anal anastomosis (IPAA) |
| Endo-GIA | Endoscopic GastrointestinalAnastomosis | Laparoscopic GIA, reloadable, articulating | Laparoscopic bowel/gastric resections |
| LCS | Linear Cutting Stapler | Linear cut + staple | GI and thoracic surgery |
| Skin stapler | — | Applies linear metallic staples to skin | Scalp, trunk, post-thoracotomy wounds |
Advantages — Mnemonic “FAST”
- F — Fast: quicker than hand suturing
- A — Atraumatic: minimal tissue handling
- S — Secure: uniform, reproducible staple line
- T — Time-saving: reduces operative duration
Additional: better haemostasis, reduced anastomotic leak rates.
Disadvantages / Complications
- Expensive; requires experience and precision
- Not ideal for very thick or oedematous tissue
- Staple-line bleeding or anastomotic leak
- Device malfunction — incomplete firing or misfire
- Stricture formation at circular anastomosis sites
Recent Advances
- Powered staplers: Battery/electronic activation — uniform compression force regardless of tissue thickness
- Articulating staplers: Adjustable angles for deep pelvic or laparoscopic work
- Smart staplers: Pressure sensors that optimise staple height based on tissue thickness
- Bioabsorbable staples: Minimal imaging interference; under investigation
Composite Meshes
►Definition
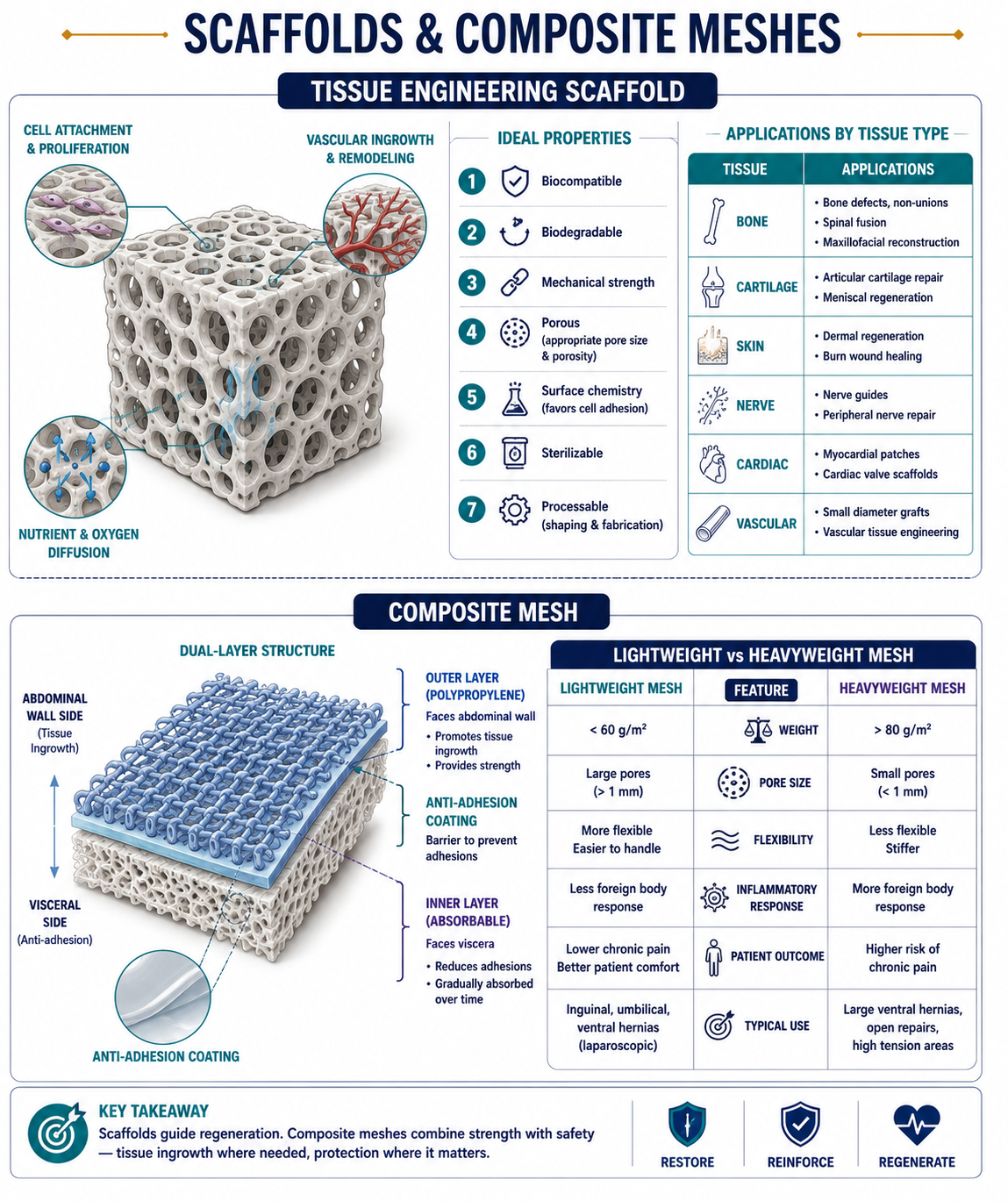
Composite meshes are dual-layer or multi-layer prosthetic materials designed for intraperitoneal hernia repair, consisting of a permanent structural layer (polypropylene) on the abdominal wall side and an anti-adhesion layer (absorbable or non-absorbable) on the visceral side to prevent bowel adhesion to the mesh.
Why Composite Meshes?
Plain polypropylene mesh in direct contact with bowel causes dense adhesions, erosion, and fistula formation. Composite meshes solve this by keeping reactive material away from the viscera.
Types / Layers
| Layer | Material | Property |
|---|---|---|
| Parietal (abdominal wall) side | Polypropylene (PP) / Polyester | Promotes fibrosis and tissue ingrowth into abdominal wall |
| Visceral side | Polytetrafluoroethylene (PTFE / ePTFE), oxidised regenerated cellulose (ORC), hyaluronate/CMC film, Omega-3 fatty acid coating | Anti-adhesion barrier; prevents bowel attachment; often absorbable over time |
Common Composite Mesh Products
- Proceed (PP + ORC + PDS film) — absorbable visceral layer
- Parietex Composite (polyester + collagen film) — excellent tissue integration
- Ventralight (PP + hydroxyethyl cellulose) — lightweight
- DualMesh (ePTFE) — smooth visceral side, microporous parietal side
- Bard Davol / Sepramesh (PP + Seprafilm derivative)
Mesh Weight Classification
| Category | Weight | Pore Size | Properties |
|---|---|---|---|
| Heavyweight | >90 g/m² | Small (<1 mm) | Strong but stiff; foreign body reaction; good for high-tension repairs |
| Lightweight | <50 g/m² | Large (>1 mm) | Flexible, less foreign body reaction; promotes better tissue integration; preferred for large defects |
| Ultralightweight | <35 g/m² | Very large | Maximum flexibility; may have lower burst strength |
Indications for Composite Mesh
- Intraperitoneal onlay mesh (IPOM) repair of ventral/incisional hernia
- Any laparoscopic ventral hernia repair where mesh contacts bowel
- Re-do hernia repair after adhesiolysis
Tissue Engineering Scaffolds
►
Definition
A scaffold in tissue engineering is a three-dimensional (3D) biocompatible structure that provides a temporary framework for cell attachment, proliferation, differentiation, and extracellular matrix (ECM) formation, ultimately guiding the regeneration of functional tissue.
Ideal Properties of a Scaffold
- Biocompatibility — must not evoke immune or inflammatory reaction
- Biodegradability — degrades at a controlled rate matching tissue formation
- Mechanical strength — adequate to withstand physiological stress
- Porosity & interconnectivity — allows nutrient diffusion, vascular ingrowth, and waste removal
- Surface chemistry — promotes cell adhesion and growth
- Sterilisability — must withstand sterilisation without altering properties
- Processability — easy to fabricate into desired shape and size
Functions
- Acts as template for tissue regeneration
- Facilitates cell attachment and migration
- Allows vascular ingrowth and nutrient diffusion
- Provides mechanical support until native tissue regenerates
- Serves as delivery system for growth factors, drugs, or genes
Applications by Tissue Type
| Tissue | Common Scaffold Type |
|---|---|
| Bone | Hydroxyapatite–PLGA, PCL, collagen composites |
| Cartilage | Alginate, chitosan, hyaluronic acid gels |
| Skin | Collagen and fibrin matrices |
| Nerve | Aligned nanofibre scaffolds |
| Vascular | Biodegradable polymer tubes (PGA, PCL) |
| Liver / Pancreas | Hydrogel or decellularised organ matrix |
Fabrication Techniques
- Solvent casting & particulate leaching — creates porous structure
- Freeze-drying (lyophilisation) — highly porous, interconnected scaffolds
- Electrospinning — produces nanofibrous mats mimicking ECM architecture
- 3D bioprinting — precise architecture with defined cell distribution
- Gas foaming / phase separation — creates pores without organic solvents
Recent Advances
- Decellularised organ scaffolds — retain natural ECM composition and architecture; used for tracheal, oesophageal, and bladder reconstruction
- Smart scaffolds — responsive to pH, temperature, or bioactive signals; release growth factors on demand
- Nanocomposite scaffolds — improved mechanical and biofunctional properties
- 3D bioprinted scaffolds — patient-specific tissue constructs with incorporated cells