Appendix
Acute appendicitis to complicated disease — pathophysiology, scoring systems, operative and non-operative management, and the evolving evidence for selective antibiotics-first treatment.
Acute Appendicitis — Pathophysiology, Diagnosis & Management
►
Definition
Acute appendicitis is acute inflammation of the vermiform appendix, most often caused by luminal obstruction, leading to progressive bacterial overgrowth, ischaemia, and potential perforation. It is the most common surgical abdominal emergency.
Etiopathogenesis
Commonest cause — luminal obstruction:
- Fecolith — most common in adults
- Lymphoid hyperplasia — common in children and young adults (10–30 yr age group)
- Rare: parasites (Enterobius vermicularis), tumours (carcinoid, adenocarcinoma), foreign body, stricture
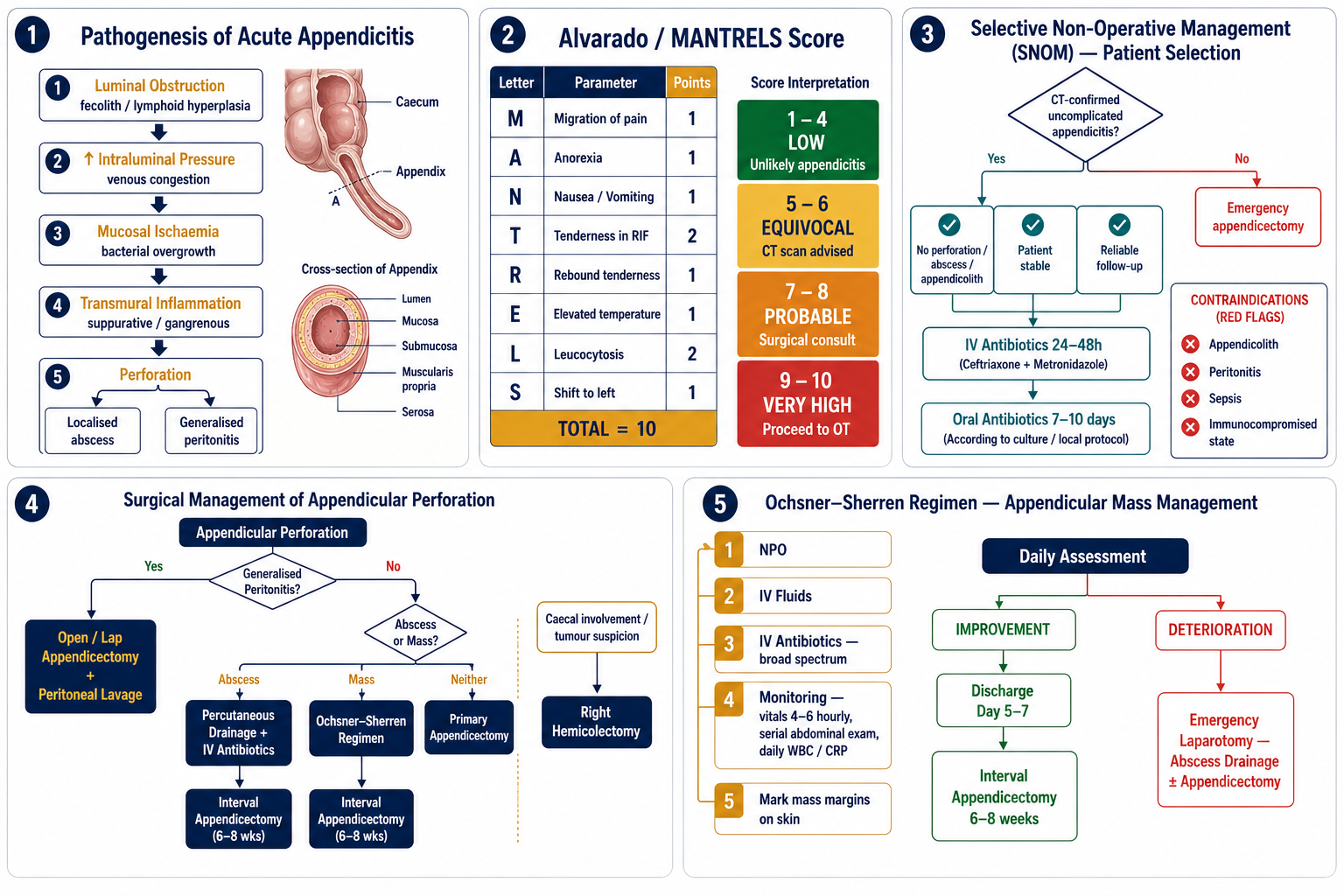
Luminal obstruction → continued mucus secretion → ↑ intraluminal pressure → venous congestion & lymphatic stasis → mucosal ischaemia → bacterial overgrowth (initially aerobic, later anaerobic) → transmural inflammation
Outcomes: Suppurative appendicitis → Gangrenous appendicitis → Perforation → Localised abscess / Generalised peritonitis
Clinical Features
Peak incidence 10–30 years; male slightly > female.
Classic symptom sequence: vague periumbilical pain (visceral, T10 dermatome) → anorexia → nausea/vomiting → migration of pain to right iliac fossa (somatic, parietal peritoneum).
Signs:
- Tenderness and guarding at McBurney’s point (RIF)
- Rebound tenderness — Blumberg sign
- Rovsing’s sign — RIF pain on palpating LIF
- Psoas sign — pain on right hip extension (retrocaecal appendix)
- Obturator sign — pain on internal rotation of flexed right hip (pelvic appendix)
- Dunphy’s sign — pain worsens on coughing
Classification
| Type | Description | Management Trend |
|---|---|---|
| Uncomplicated | Inflamed appendix, no perforation or abscess | Surgery or antibiotics-first |
| Complicated | Perforation, abscess, phlegmon, peritonitis | Drainage ± delayed surgery |
Investigations
Laboratory: CBC — leucocytosis (10,000–18,000/mm³, neutrophilia); CRP elevated in later stages; urinalysis to exclude UTI/ureteric colic.
Imaging:
- USG abdomen: Non-compressible blind-ended tubular structure >6 mm diameter; wall thickening, periappendiceal fluid, appendicolith
- CT abdomen (gold standard in adults): Dilated appendix >6 mm, wall enhancement, periappendiceal fat stranding, abscess, perforation
- MRI: Useful in pregnancy (radiation-free)
- Plain X-ray: Limited role; may reveal fecolith or ileus
Differential Diagnosis
- Mesenteric adenitis
- Gastroenteritis
- UTI / ureteric colic
- Ovarian torsion / ectopic pregnancy (females)
- Meckel’s diverticulitis
Management
Initial resuscitation: NPO; IV fluids; IV antibiotics (broad-spectrum — cover Gram-negatives and anaerobes, e.g., ceftriaxone + metronidazole); analgesics/antipyretics.
1. Uncomplicated acute appendicitis — Appendectomy
| Approach | Details | Advantages |
|---|---|---|
| Open Appendectomy | McBurney’s (gridiron) or Lanz incision → muscle splitting → isolate appendix → ligate mesoappendix (appendicular artery) → ligate and remove appendix → close stump (simple ligation ± invagination) | Short operative time, minimal equipment, useful in resource-limited settings |
| Laparoscopic Appendectomy | 3-port technique; preferred in obese, young females, diagnostic uncertainty | Less pain, shorter hospital stay, early return to work, better cosmesis, whole abdomen visualisation |
2. Conservative management (Antibiotics first) — selected cases
- High-risk patients unfit for anaesthesia/surgery
- Protocol: IV antibiotics + observation
- Drawback: Recurrence in 15–30% within 1 year
- Still controversial (Bailey & Love, Sabiston)
Postoperative Care
- Analgesia; antibiotics if perforated or suppurative
- Early ambulation, early oral intake (ERAS principles)
- Wound care
Complications of Appendicectomy
Early: Wound infection (most common complication), intra-abdominal abscess (pelvic, subphrenic, interloop), paralytic ileus, sepsis.
Late: Adhesive intestinal obstruction, incisional hernia (rare with laparoscopy), fistula (rare — stump blow-out in perforated cases).
Alvarado / MANTRELS Scoring System
►Purpose
A clinical scoring system designed to improve diagnostic accuracy and reduce unnecessary appendicectomies or missed diagnoses. Score ≥7 strongly suggests acute appendicitis.
Components — MANTRELS Mnemonic
| Letter | Feature | Points |
|---|---|---|
| M | Migration of pain to RIF | 1 |
| A | Anorexia | 1 |
| N | Nausea / Vomiting | 1 |
| T | Tenderness in RIF | 2 |
| R | Rebound tenderness (Blumberg sign) | 1 |
| E | Elevated temperature (>37.3°C) | 1 |
| L | Leucocytosis (WBC >10,000) | 2 |
| S | Shift to left (neutrophilia) | 1 |
| Total | 10 | |
Interpretation
| Score | Interpretation | Action |
|---|---|---|
| 1–4 | Low probability | Discharge / observe |
| 5–6 | Equivocal | CT scan / further observation |
| 7–8 | Probable appendicitis | Surgical consultation; consider OT |
| 9–10 | Very high probability | Proceed to appendicectomy |
AIR Score
The Appendicitis Inflammatory Response (AIR) score is a more recent alternative that incorporates CRP in addition to clinical features, improving discriminatory power particularly in the equivocal range. Both scores are currently in clinical use.
Selective Non-Operative Management (SNOM) — Recent Advances
►Concept
SNOM refers to the management of CT-confirmed uncomplicated acute appendicitis with antibiotics alone, without immediate surgical intervention. Supported by RCTs (APPAC, CODA trials) as a viable alternative to appendicectomy in selected patients.
Indications (patient must fulfil ALL criteria)
- CT-confirmed uncomplicated appendicitis
- No perforation, abscess, or appendicolith
- Patient stable, compliant, and reliable follow-up available
Contraindications
- Appendicolith present (↑ recurrence and failure rate)
- Peritonitis, sepsis, perforation, abscess
- Immunocompromised status or pregnancy (relative)
Antibiotic Protocol
↓
Oral phase (7–10 days): Levofloxacin + Metronidazole
Outcomes & Limitations
- Success rate: ~70–75% in carefully selected patients at 1 year
- Recurrence rate: 15–30% within 1 year after initially successful SNOM
- Appendicolith strongly predicts failure — avoid SNOM if present
- Patients must be counselled about recurrence and need for eventual appendicectomy
MIS & ERAS Integration
| Innovation | Concept | Status |
|---|---|---|
| Same-Day (Ambulatory) Appendectomy | For stable, young, uncomplicated cases; discharge within 12 hrs with early feeding and ambulation (ERAS principles) | Supported |
| Single Incision Laparoscopic Appendectomy (SILA) | Cosmetically superior; same outcomes | Select centres |
| NOTES (Natural Orifice Transluminal Endoscopic Surgery) | Transvaginal/transgastric approach | Experimental |
| ERAT (Endoscopic Retrograde Appendicitis Therapy) | Colonoscopic drainage + stenting of appendix | Promising; investigational |
| Telemedicine follow-up | Early monitoring, fewer readmissions post-SNOM | Increasingly used |
Appendicular Perforation
►Definition
Appendicular perforation refers to full-thickness necrosis of the appendix wall with release of luminal contents into the peritoneal cavity, resulting in localised or generalised peritonitis.
Classification by Clinical Presentation
| Type | Features |
|---|---|
| Localised perforation | Walled-off by omentum → phlegmon or abscess |
| Generalised peritonitis | Free perforation with faecal contamination |
| Appendicular mass | Inflamed appendix with surrounding inflammatory mass |
| Appendicular abscess | Localised collection due to perforation |
Surgical Options
A. Emergency Appendectomy
Indication: Generalised peritonitis or uncontained perforation.
- Open appendectomy: Preferred in generalised peritonitis; lower risk of intra-abdominal sepsis in contaminated field
- Laparoscopic appendectomy: Selected cases (stable patient, localised contamination); offers earlier recovery but may increase intra-abdominal abscess risk in perforated cases
B. Drainage + Delayed (Interval) Appendectomy
Indication: Appendicular abscess or mass with a stable patient and no generalised peritonitis.
- Percutaneous or open drainage of abscess + broad-spectrum antibiotics
- Interval appendectomy after 6–8 weeks (controversial — some advocate observation if subsequently asymptomatic)
C. Resectional Surgery
Indication: Extensive local necrosis, caecal involvement, or intraoperative suspicion of neoplasm.
- Ileocaecal resection or right hemicolectomy
- Indicated when base necrosis involves caecum, large perforation not amenable to simple appendicectomy, or intraoperative malignancy concern
Surgical Decision Algorithm
| Clinical Scenario | Surgical Option |
|---|---|
| Generalised peritonitis | Open or laparoscopic appendectomy ± peritoneal lavage |
| Localised abscess (stable patient) | Image-guided drainage ± interval appendectomy |
| Appendicular mass (conservative) | Ochsner–Sherren regimen ± interval appendectomy |
| Extensive caecal involvement / necrosis | Ileocaecal resection or right hemicolectomy |
| Intraoperative suspicion of tumour | Oncological right hemicolectomy |
Perioperative Considerations
- Antibiotics: Broad-spectrum covering Gram-negatives and anaerobes (e.g., piperacillin–tazobactam or ceftriaxone + metronidazole)
- Peritoneal lavage: Especially in faecal peritonitis
- Drain placement: Controversial; individualised based on degree of contamination
Postoperative Complications
- Intra-abdominal abscess
- Wound infection
- Enterocutaneous fistula (rare)
- Prolonged ileus
Appendicular Mass & Abscess — Ochsner–Sherren Regimen
►Appendicular Mass
Pathology: Inflamed appendix + omentum + adjacent bowel wall forming a palpable mass after 48–72 hours of symptoms. Not yet a frank abscess — no drainable collection.
Ochsner–Sherren Regimen (Conservative Management)
- Nil per oral (NPO)
- IV fluids (correct dehydration and electrolyte imbalance)
- IV antibiotics (broad-spectrum: Gram-negatives + anaerobes)
- Strict monitoring: vitals every 4–6 hrs, serial abdominal examinations, daily WBC and CRP
- Mark the mass margins on the skin with a skin marker — monitor for change in size
Decision Points During Regimen
| Finding | Action |
|---|---|
| Improvement (mass reduces, fever settles, WBC falling) | Continue conservative; discharge after 5–7 days → Interval appendicectomy at 6–8 weeks |
| Deterioration (fever worsens, mass increases, signs of peritonitis) | Emergency laparotomy: abscess drainage ± appendicectomy |
| Abscess formation (USG/CT confirms collection) | Percutaneous image-guided drainage + antibiotics; interval appendicectomy later |
Interval Appendicectomy
- Performed electively 6–8 weeks after resolution of appendicular mass
- Controversial: some centres advocate observation if the patient is asymptomatic after resolution
- Indications to proceed even if asymptomatic: age >40 years (to exclude underlying tumour), appendicolith on imaging, recurrent symptoms
Appendicular Abscess
Definition: Localised collection of pus (confirmed on USG or CT) resulting from a walled-off perforation.
Management:
- First line: USG/CT-guided percutaneous drainage + IV antibiotics
- Definitive: Interval appendicectomy after 6–8 weeks
- Open drainage if percutaneous not feasible or patient deteriorates
Key Exam Pearls
- Appendicectomy is the gold standard treatment for acute appendicitis
- Appendicular mass → conservative (Ochsner–Sherren) first, then interval appendicectomy
- Abscess → percutaneous drainage + antibiotics; appendicectomy deferred
- Perforated appendicitis with generalised peritonitis → emergency surgery without delay
- Laparoscopic approach increasingly preferred, but open appendicectomy remains valid in generalised contamination
- Intraoperative suspicion of tumour → right hemicolectomy, not simple appendicectomy